

Clinical review: What are the best hemodynamic targets for noncardiac surgical patients?
- PMID: 23672840
- PMCID: PMC3672542
- DOI: 10.1186/cc11861
Clinical review: What are the best hemodynamic targets for noncardiac surgical patients?
Abstract
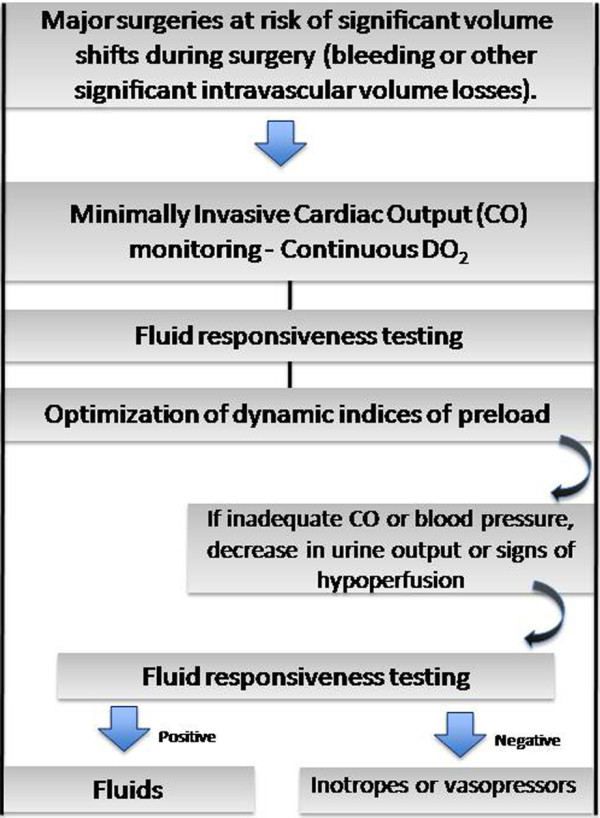
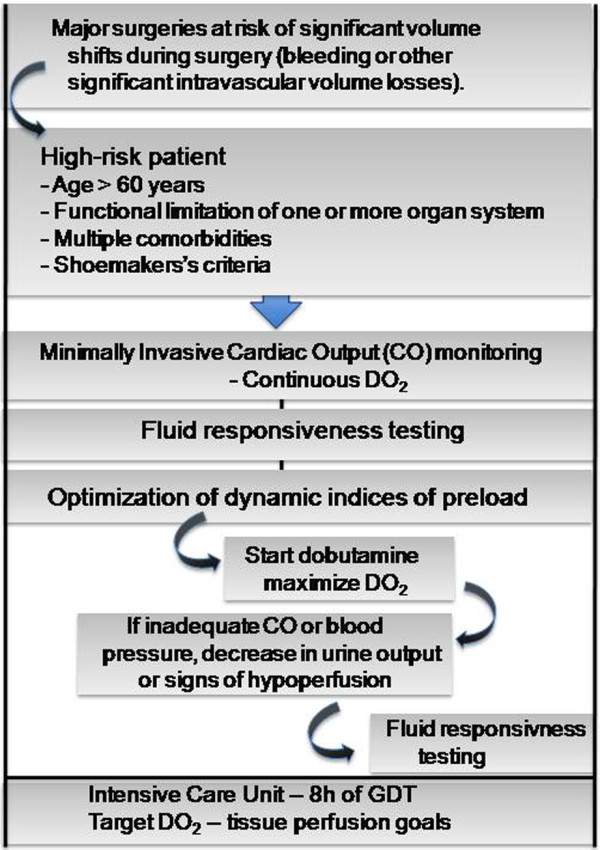
Perioperative hemodynamic optimization, or goal-directed therapy (GDT), has been show to significantly decrease complications and risk of death in high-risk patients undergoing noncardiac surgery. An important aim of GDT is to prevent an imbalance between oxygen delivery and oxygen consumption in order to avoid the development of multiple organ dysfunction. The utilization of cardiac output monitoring in the perioperative period has been shown to improve outcomes if integrated into a GDT strategy. GDT guided by dynamic predictors of fluid responsiveness or functional hemodynamics with minimally invasive cardiac output monitoring is suitable for the majority of patients undergoing major surgery with expected significant volume shifts due to bleeding or other significant intravascular volume losses. For patients at higher risk of complications and death, such as those with advanced age and limited cardiorespiratory reserve, the addition of dobutamine or dopexamine to the treatment algorithm, to maximize oxygen delivery, is associated with better outcomes.
Figures
References
-
- Lobo SM, Rezende E, Knibel MF, Silva NB, Páramo JA, Nácul FE, Mendes CL, Assunção M, Costa RC, Grimm CC, Pinto SF, Mello PM, Maia MO, Duarte PA, Gutierrez F, Silva JM Jr, Lopes MR, Cordeiro JA, Mellot C. Early determinants of death due to multiple organ failure after non cardiac surgery in high-risk patients. Anesth Analg. 2011;112:877–883. doi: 10.1213/ANE.0b013e3181e2bf8e. - DOI - PubMed
-
- Shoemaker WC, Montgomery ES, Kaplan E, Elwyn DW. Physiologic patterns in surviving and nonsurviving shock patients. Use of sequential cardiorespiratory variables in defining criteria for therapeutic goals and early warning of death. Arch Surg. 1993;106:630–636. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
