

The use of CT findings to predict extent of tumor at primary surgery for ovarian cancer
- PMID: 23672930
- PMCID: PMC3753038
- DOI: 10.1016/j.ygyno.2013.05.007
The use of CT findings to predict extent of tumor at primary surgery for ovarian cancer
Abstract
Background: High tumor dissemination (HTD) is a major risk factor for serious morbidity after primary ovarian cancer (OC) surgery, particularly in medically compromised patients. We performed a pilot study of whether CT findings could predict extent of disease and surgical complexity necessary in advanced OC.
Methods: Preoperative CT images for patients with advanced OC from 1997-2003 were evaluated for rigorously defined disease-related findings and compared to both the findings at exploration and the required surgical procedures. Associations were assessed by the chi-square test.
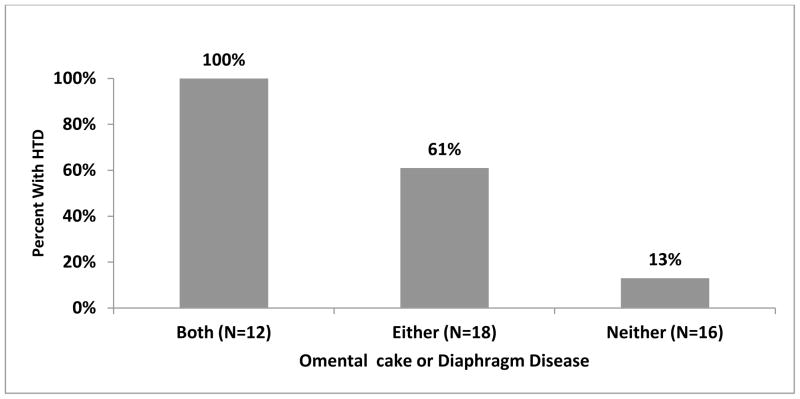
Results: Forty-six cases met inclusion criteria. Mean age was 66.4y, and 76% had residual disease (RD) 1cm or less. CT and surgical findings correlated (sensitivity/specificity) as follows: diaphragm disease (48%/100%); surface liver (100%/93%); omental cake (72%/65%); any sigmoid involvement (54%/100%); ascites (44%/100%); extra-pelvic large bowel involvement (29%/91%). When diaphragm disease and omental cake were present, HTD was found in all cases (positive predictive value and specificity=100%, sensitivity 48%). For CT findings of liver, large bowel and spleen involvement there was a strong trend toward resection (P=0.001, P=0.06 and P=0.06, respectively).
Conclusions: The findings of diaphragm disease and omental cake on CT scan are highly predictive for high tumor dissemination (HTD) and thus likelihood of extensive surgery required to achieve low residual disease. In addition, multiple CT findings correlate strongly with the need for higher surgical complexity which should facilitate preoperative planning and/or triage to specialized centers. These preliminary data suggest specific CT findings can be used to optimize treatment planning.
Keywords: Cytoreduction; Outcome assessment; Ovarian neoplasms; Radiologic imaging.
Copyright © 2013 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Hennessy BT, Coleman RL, Markman M. Ovarian cancer. Lancet. 2009;374:1371–82. - PubMed
-
- Morgan RJ, Jr, Alvarez RD, Armstrong DK, Boston B, Chen LM, Copeland L, Fowler J, Gaffney DK, Gershenson D, Greer BE, Grigsby PW, Havrilesky LJ, Johnston C, Lancaster JM, Lele S, Matulonis U, O’Malley D, Ozols RF, Remmenga SW, Sabbatini P, Schink J, Teng N. Ovarian cancer. Clinical practice guidelines in oncology. Journal of the National Comprehensive Cancer Network: JNCCN. 2008;6:766–94. - PubMed
-
- McGuire WP, Hoskins WJ, Brady MF, Kucera PR, Partridge EE, Look KY, Clarke-Pearson DL, Davidson M. Cyclophosphamide and cisplatin compared with paclitaxel and cisplatin in patients with stage III and stage IV ovarian cancer. The New England journal of medicine. 1996;334:1–6. - PubMed
-
- Ozols RF, Bundy BN, Greer BE, Fowler JM, Clarke-Pearson D, Burger RA, Mannel RS, DeGeest K, Hartenbach EM, Baergen R. Phase III trial of carboplatin and paclitaxel compared with cisplatin and paclitaxel in patients with optimally resected stage III ovarian cancer: a Gynecologic Oncology Group study. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2003;21:3194–200. - PubMed
-
- Aletti GD, Dowdy SC, Podratz KC, Cliby WA. Relationship among surgical complexity, short-term morbidity, and overall survival in primary surgery for advanced ovarian cancer. American journal of obstetrics and gynecology. 2007;197:676, e1–7. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
