The benefit of intraperitoneal chemotherapy for the treatment of colorectal carcinomatosis
- PMID: 23673557
- PMCID: PMC3729245
- DOI: 10.3892/or.2013.2473
The benefit of intraperitoneal chemotherapy for the treatment of colorectal carcinomatosis
Abstract
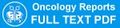
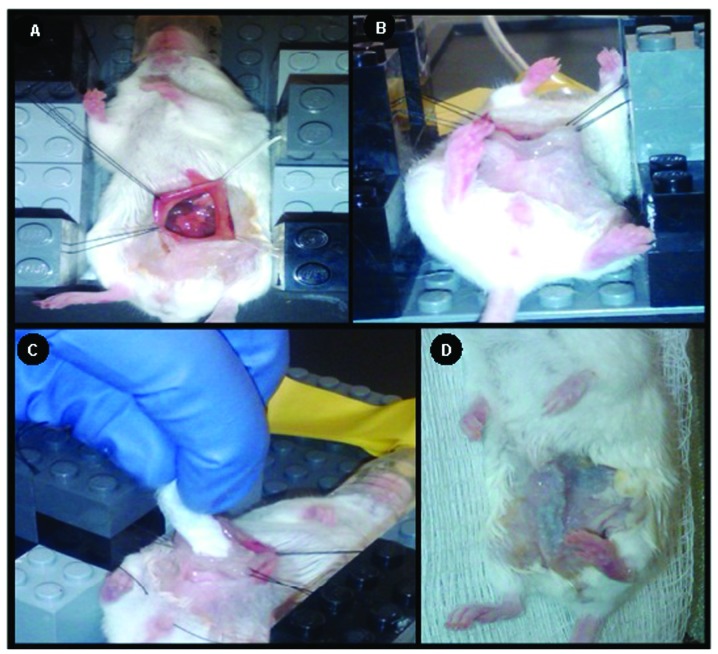
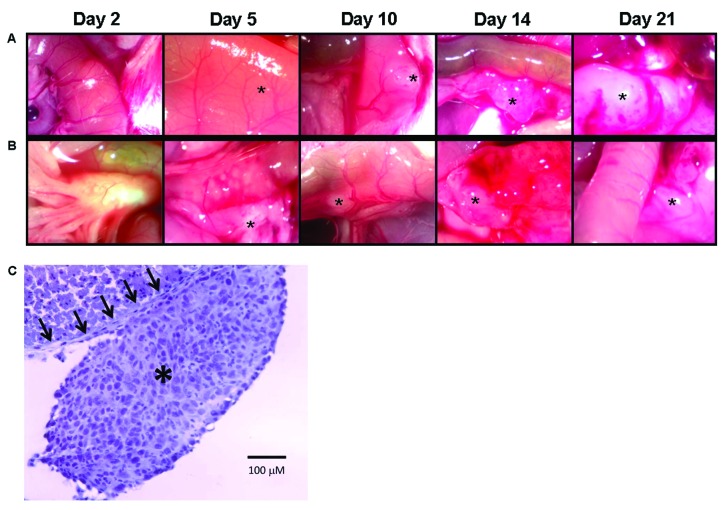
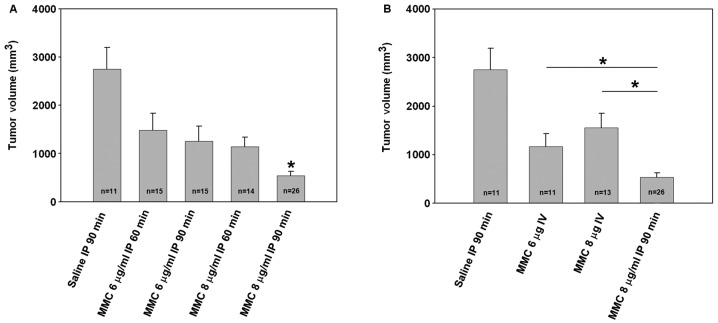
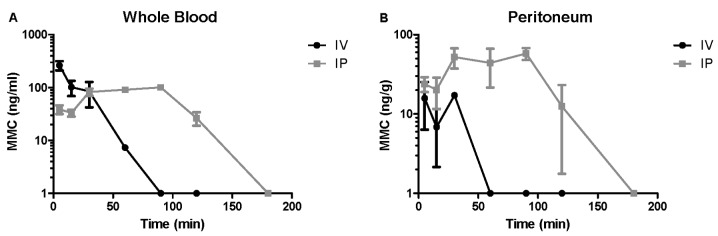
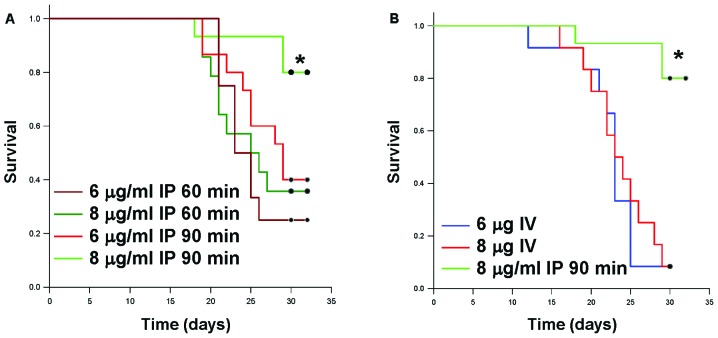
The clinical practice of hyperthermic intraperitoneal chemoperfusion (HIPEC) for carcinomatosis has lacked preclinical justification. A standardized mouse model was created to evaluate the independent effects of intraperitoneal chemotherapy. Diffuse colorectal carcinomatosis was generated in mice prior to intraperitoneal lavage with mitomycin C (MMC) at clinically comparable dosing for variable lengths of time. Tumor volumes, MMC tissue concentrations and survival were measured in comparison to saline lavage and intravenous MMC. Magnetic resonance imaging revealed a direct correlation between tumor volume, MMC dose and exposure time and survival. Intravenous MMC demonstrated a rapid clearance from the blood, lower peritoneal tissue concentrations, less tumor growth inhibition and decreased survival compared to intraperitoneal administration. Intraperitoneal chemotherapy inhibited tumor growth independent of cytoreduction or hyperthermia, demonstrated improved peritoneal tissue concentration and was associated with increased survival. These data support the clinical utility of the intraperitoneal chemotherapy component of HIPEC.
Figures
References
-
- Siegel R, DeSantis C, Virgo K, et al. Cancer treatment and survivorship statistics, 2012. CA Cancer J Clin. 2012;62:220–241. - PubMed
-
- Chu DZ, Lang NP, Thompson C, Osteen PK, Westbrook KC. Peritoneal carcinomatosis in nongynecologic malignancy. A prospective study of prognostic factors. Cancer. 1989;63:364–367. - PubMed
-
- Elias D, Delperro JR, Sideris L, et al. Treatment of peritoneal carcinomatosis from colorectal cancer: impact of complete cytoreductive surgery and difficulties in conducting randomized trials. Ann Surg Oncol. 2004;11:518–521. - PubMed
-
- Sugarbaker PH. A curative approach to peritoneal carcinomatosis from colorectal cancer. Semin Oncol. 2005;32:S68–S73. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical