

Effect of a course-based intervention and effect of medical regulation on physicians' opioid prescribing
- PMID: 23673603
- PMCID: PMC3653672
Effect of a course-based intervention and effect of medical regulation on physicians' opioid prescribing
Abstract
Objective: To examine the effects of an intensive 2-day course on physicians' prescribing of opioids.
Design: Population-based retrospective observational study.
Setting: College of Physicians and Surgeons of Ontario (CPSO) in Toronto.
Participants: Ontario physicians who took the course between April 1, 2000, and May 30, 2008.
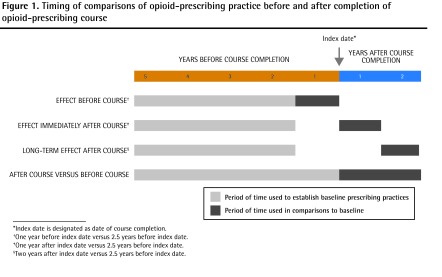
Intervention: A 2-day opioid-prescribing course with a maximum of 12 physician participants. Educational methods included didactic presentations, case discussions, and standardized patients. A detailed syllabus and office materials were provided.
Main outcome measures: Participants were matched with control physicians using specific variables. The primary outcome was the rate of opioid prescribing, expressed as milligrams of morphine equivalent per quarter.
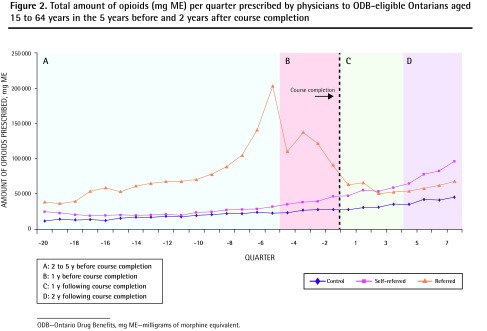
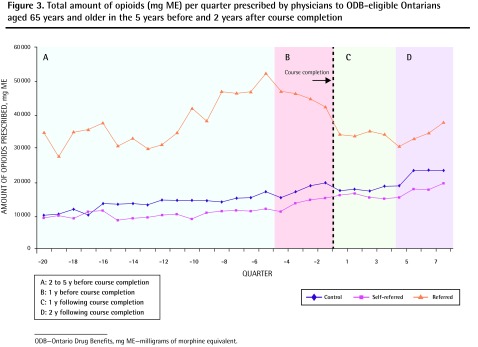
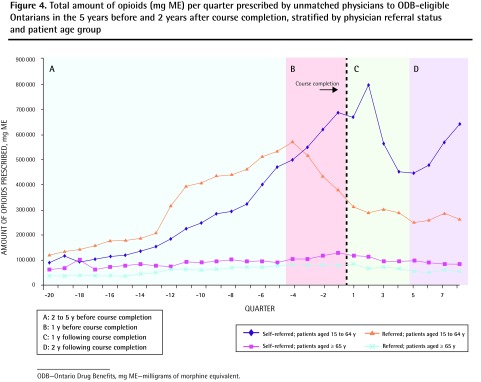
Results: One hundred thirty-eight course participants (120 family physicians, 15 specialists, and 3 physicians whose status was uncertain) were eligible for analysis. Of these, 68.1% were self-referred and 31.9% were referred by the CPSO. Overall, among physicians referred by the CPSO, the rate of opioid prescribing decreased dramatically in the year before course participation compared with matched control physicians. The course had no added effect on the rate of physicians' opioid prescribing in the subsequent 2 years. There was no statistically significant effect on the rate of opioid prescribing observed among the self-referred physicians. Among 15 of the self-referred physicians who, owing to the high quantities of opioids they prescribed, were not matched with control physicians, the rate of opioid prescribing decreased by 43.9% in the year following course completion.
Conclusion: Physicians markedly reduced the quantities of opioids they prescribed after medical regulators referred them to an opioid-prescribing course. The course itself did not lead to significant additional reductions; however, a subgroup of physicians who prescribed high quantities of opioids might have responded to what was taught in the course.
Objectif: Évaluer l’effet d’un cours intensif de 2 heures sur la prescription d’opiacés par des médecins.
Type d’étude: Étude d’observation stratifiée et rétrospective.
Contexte: L’Ordre des médecins et chirurgiens de l’Ontario (OMCO).
Participants: Médecins ontariens ayant suivi le cours entre le 1er avril 2000 et le 30 mai 2008.
Intervention: Un cours de 2 jours sur la prescription d’opiacés, réunissant un maximum de 12 médecins. Les méthodes d’enseignement comprenaient des cours magistraux, des discussions de cas et des patients types. On fournissait aussi un plan de cours et du matériel de bureau.
Principaux paramètres à l’étude: Les participants étaient appariés à des médecins témoins selon des critères spécifiques. L’issue principale était le taux de prescription d’opiacés, exprimé en milligrammes de morphine par trimestre.
Résultats: Un total de 138 médecins ayant suivi le cours (120 médecins de famille, 15 spécialistes et 3 médecins au statut incertain) étaient admissibles pour l’analyse. De ceux-là, 68,1 % participaient de façon volontaire et 31,9 %, à la demande de l’OMCO. Par rapport aux médecins témoins appariés, le taux global de prescription d’opiacés chez les médecins désignés par l’OMCO avait diminué de façon dramatique dans l’année précédant leur participation au cours. Le cours n’a eu aucun effet additionnel sur le taux de prescription des médecins au cours des 2 années subséquentes. Chez les médecins participant de façon volontaire, on n’a observé aucun effet statistiquement significatif sur le taux de prescription d’opiacés. Toutefois, chez 15 de ces derniers qui, en raison de la grande quantité d’opiacés qu’ils prescrivaient, n’avaient pas été appariés à des médecins témoins, le taux de prescription d’opiacés a diminué de 43,9 % dans l’année suivant la fin du cours.
Conclusion: On a observé une diminution importante de la quantité d‘opiacés prescrits chez les médecins après qu’ils eurent été incités par les responsables de la réglementation à suivre un cours sur la prescription d’opiacés. Le cours en soi n’a entraîné aucune diminution additionnelle; toutefois, un sous-groupe de médecins qui prescrivaient de grandes quantités d’opiacés pourrait avoir répondu positivement aux notions enseignées dans le cours.
Figures
References
-
- Fischer B, Nakamura N, Rush B, Rehm J, Urbanoski K. Changes in and characteristics of admissions to treatment related to problematic prescription opioid use in Ontario, 2004–2009. Drug Alcohol Depend. 2010;109(1–3):257–60. Epub 2010 Mar 1. - PubMed
-
- Sproule B, Brands B, Li S, Catz-Biro L. Changing patterns in opioid addiction. Characterizing users of oxycodone and other opioids. Can Fam Physician. 2009;55:68-9.e1–5. Available from: www.cfp.ca/content/55/1/68.full.pdf+html. Accessed 2013 Apr 11. - PMC - PubMed
-
- College of Physicians and Surgeons of Ontario . Avoiding abuse, achieving a balance: tackling the opioid public health crisis. Toronto, ON: College of Physicians and Surgeons of Ontario; 2010. Available from: www.cpso.on.ca/uploadedFiles/policies/positions/Opioid%20report%20final.pdf. Accessed 2013 Apr 11.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous