

Effects of Nigella sativa on outcome of hepatitis C in Egypt
- PMID: 23674855
- PMCID: PMC3646144
- DOI: 10.3748/wjg.v19.i16.2529
Effects of Nigella sativa on outcome of hepatitis C in Egypt
Abstract
Aim: To evaluate the safety, efficacy and tolerability of Nigella sativa (N. sativa) in patients with hepatitis C not eligible for interferon (IFN)-α.
Methods: Thirty patients with hepatitis C virus (HCV) infection, who were not eligible for IFN/ribavirin therapy, were included in the present study. Inclusion criteria included: patients with HCV with or without cirrhosis, who had a contraindication to IFN-α therapy, or had refused or had a financial constraint to IFN-α therapy. Exclusion criteria included: patients on IFN-α therapy, infection with hepatitis B or hepatitis I virus, hepatocellular carcinoma, other malignancies, major severe illness, or treatment non-compliance. Various parameters, including clinical parameters, complete blood count, liver function, renal function, plasma glucose, total antioxidant capacity (TAC), and polymerase chain reaction, were all assessed at baseline and at the end of the study. Clinical assessment included: hepato and/or splenomegaly, jaundice, palmar erythema, flapping tremors, spider naevi, lower-limb edema, and ascites. N. sativa was administered for three successive months at a dose of (450 mg three times daily). Clinical response and incidence of adverse drug reactions were assessed initially, periodically, and at the end of the study.
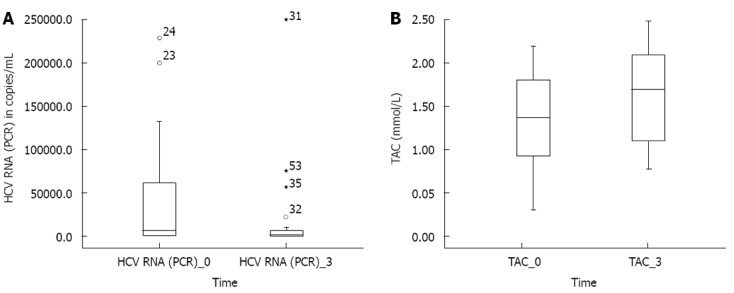
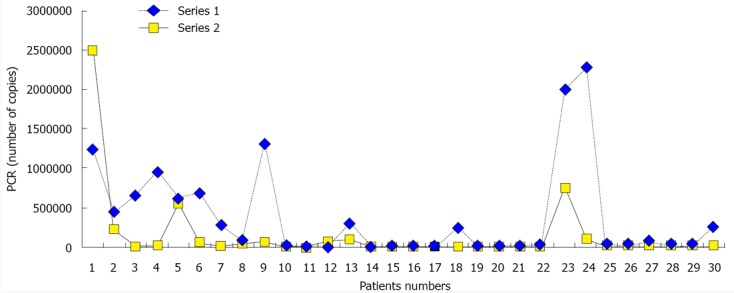
Results: N. sativa administration significantly improved HCV viral load (380808.7 ± 610937 vs 147028.2 ± 475225.6, P = 0.001) and TAC (1.35 ± 0.5 vs 1.612 ± 0.56, P = 0.001). After N. sativa administration, the following laboratory parameters improved: total protein (7.1 ± 0.7 vs 7.5 ± 0.8, P = 0.001), albumin (3.5 ± 0.87 vs 3.69 ± 0.91, P = 0.008), red blood cell count (4.13 ± 0.9 vs 4.3 ± 0.9, P = 0.001), and platelet count (167.7 ± 91.2 vs 198.5 ± 103, P = 0.004). Fasting blood glucose (104.03 ± 43.42 vs 92.1 ± 31.34, P = 0.001) and postprandial blood glucose (143.67 ± 72.56 vs 112.1 ± 42.9, P = 0.001) were significantly decreased in both diabetic and non-diabetic HCV patients. Patients with lower-limb edema decreased significantly from baseline compared with after treatment [16 (53.30%) vs 7 (23.30%), P = 0.004]. Adverse drug reactions were unremarkable except for a few cases of epigastric pain and hypoglycemia that did not affect patient compliance.
Conclusion: N. sativa administration in patients with HCV was tolerable, safe, decreased viral load, and improved oxidative stress, clinical condition and glycemic control in diabetic patients.
Keywords: Hepatitis C virus; Nigella sativa; Oxidative stress; Viral load.
Figures
References
-
- Nguyen MH, Keeffe EB. Prevalence and treatment of hepatitis C virus genotypes 4, 5, and 6. Clin Gastroenterol Hepatol. 2005;3:S97–S101. - PubMed
-
- Abdel-Aziz F, Habib M, Mohamed MK, Abdel-Hamid M, Gamil F, Madkour S, Mikhail NN, Thomas D, Fix AD, Strickland GT, et al. Hepatitis C virus (HCV) infection in a community in the Nile Delta: population description and HCV prevalence. Hepatology. 2000;32:111–115. - PubMed
-
- Elkady A, Tanaka Y, Kurbanov F, Sugauchi F, Sugiyama M, Khan A, Sayed D, Moustafa G, Abdel-Hameed AR, Mizokami M. Genetic variability of hepatitis C virus in South Egypt and its possible clinical implication. J Med Virol. 2009;81:1015–1023. - PubMed
-
- Khattab MA, Ferenci P, Hadziyannis SJ, Colombo M, Manns MP, Almasio PL, Esteban R, Abdo AA, Harrison SA, Ibrahim N, et al. Management of hepatitis C virus genotype 4: recommendations of an international expert panel. J Hepatol. 2011;54:1250–1262. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
