

Narrow-band imaging with magnifying endoscopy is accurate for detecting gastric intestinal metaplasia
- PMID: 23674874
- PMCID: PMC3645385
- DOI: 10.3748/wjg.v19.i17.2668
Narrow-band imaging with magnifying endoscopy is accurate for detecting gastric intestinal metaplasia
Abstract
Aim: To investigate the predictive value of narrow-band imaging with magnifying endoscopy (NBI-ME) for identifying gastric intestinal metaplasia (GIM) in unselected patients.
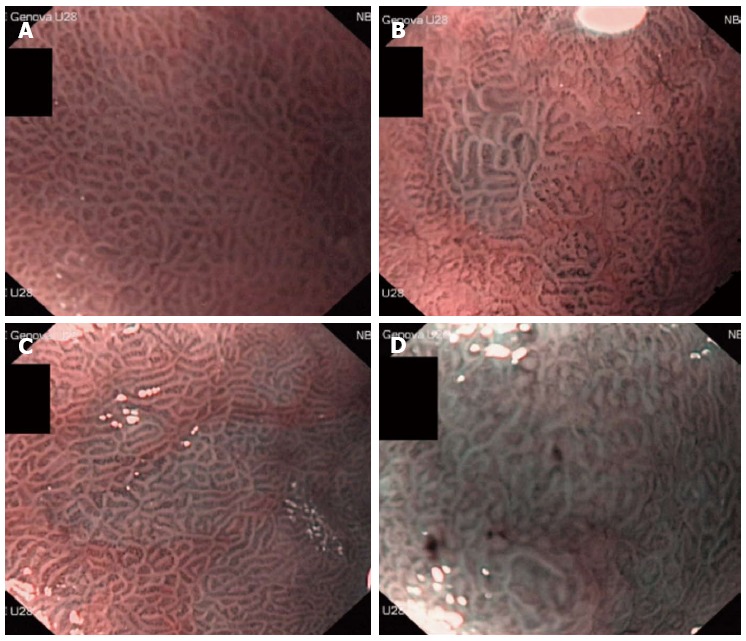
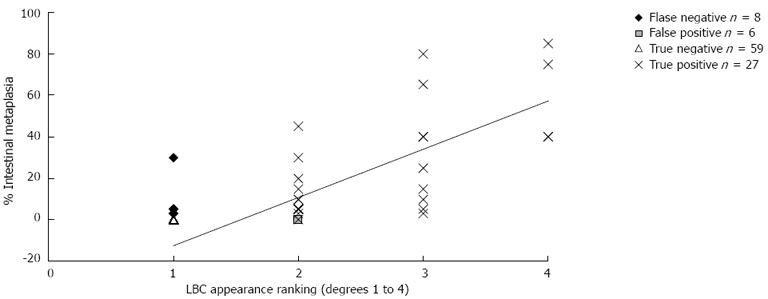
Methods: We prospectively evaluated consecutive patients undergoing upper endoscopy for various indications, such as epigastric discomfort/pain, anaemia, gastro-oesophageal reflux disease, suspicion of peptic ulcer disease, or chronic liver diseases. Patients underwent NBI-ME, which was performed by three blinded, experienced endoscopists. In addition, five biopsies (2 antrum, 1 angulus, and 2 corpus) were taken and examined by two pathologists unaware of the endoscopic findings to determine the presence or absence of GIM. The correlation between light blue crest (LBC) appearance and histology was measured. Moreover, we quantified the degree of LBC appearance as less than 20% (+), 20%-80% (++) and more than 80% (+++) of an image field, and the semiquantitative evaluation of LBC appearance was correlated with IM percentage from the histological findings.
Results: We enrolled 100 (58 F/42 M) patients who were mainly referred for gastro-esophageal reflux disease/dyspepsia (46%), cancer screening/anaemia (34%), chronic liver disease (9%), and suspected celiac disease (6%); the remaining patients were referred for other indications. The prevalence of Helicobacter pylori (H. pylori) infection detected from the biopsies was 31%, while 67% of the patients used proton pump inhibitors. LBCs were found in the antrum of 33 patients (33%); 20 of the cases were classified as LBC+, 9 as LBC++, and 4 as LBC+++. LBCs were found in the gastric body of 6 patients (6%), with 5 of them also having LBCs in the antrum. The correlation between the appearance of LBCs and histological GIM was good, with a sensitivity of 80% (95%CI: 67-92), a specificity of 96% (95%CI: 93-99), a positive predictive value of 84% (95%CI: 73-96), a negative predictive value of 95% (95%CI: 92-98), and an accuracy of 93% (95%CI: 90-97). The NBI-ME examination overlooked GIM in 8 cases, but the GIM was less than 5% in 7 of the cases. Moreover, in the 6 false positive cases, the histological examination showed the presence of reactive gastropathy (4 cases) or H. pylori active chronic gastritis (2 cases). The semiquantitative correlation between the rate of LBC appearance and the percentage of GIM was 79% (P < 0.01).
Conclusion: NBI-ME achieved good sensitivity and specificity in recognising GIM in an unselected population. In routine clinical practice, this technique can reliably target gastric biopsies.
Keywords: Endoscopy; Gastric biopsy; Gastric cancer; Gastric intestinal metaplasia; Light blue crest; Magnification; Narrow-band imaging; Precancerous conditions.
Figures
References
-
- de Vries AC, Haringsma J, Kuipers EJ. The detection, surveillance and treatment of premalignant gastric lesions related to Helicobacter pylori infection. Helicobacter. 2007;12:1–15. - PubMed
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- Correa P. Human gastric carcinogenesis: a multistep and multifactorial process--First American Cancer Society Award Lecture on Cancer Epidemiology and Prevention. Cancer Res. 1992;52:6735–6740. - PubMed
-
- Busuttil RA, Boussioutas A. Intestinal metaplasia: a premalignant lesion involved in gastric carcinogenesis. J Gastroenterol Hepatol. 2009;24:193–201. - PubMed
-
- Inghelmann R, Grande E, Francisci S, Verdecchia A, Micheli A, Baili P, Capocaccia R, De Angelis R. Regional estimates of stomach cancer burden in Italy. Tumori. 2007;93:367–373. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
