

Evaluation of drug-induced sleep endoscopy as a patient selection tool for implanted upper airway stimulation for obstructive sleep apnea
- PMID: 23674933
- PMCID: PMC3629316
- DOI: 10.5664/jcsm.2658
Evaluation of drug-induced sleep endoscopy as a patient selection tool for implanted upper airway stimulation for obstructive sleep apnea
Abstract
Study objectives: To study the possible predictive value of drug-induced sleep endoscopy (DISE) in assessing therapeutic response to implanted upper airway stimulation (UAS) for obstructive sleep apnea (OSA).
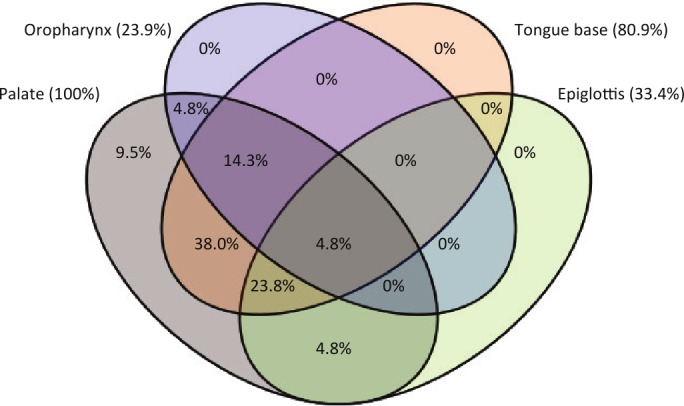
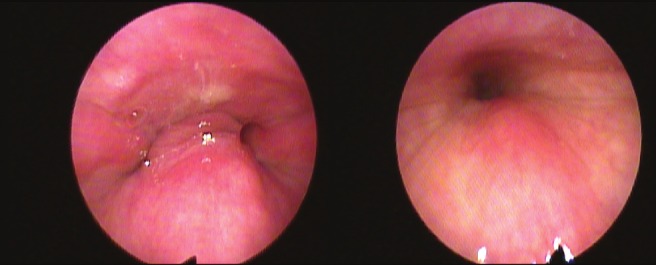
Methods: During DISE, artificial sleep is induced by midazolam and/or propofol, and the pharyngeal collapse patterns are visualized using a flexible fiberoptic nasopharyngoscope. The level (palate, oropharynx, tongue base, hypopharynx/epiglottis), the direction (anteroposterior, concentric, lateral), and the degree of collapse (none, partial, or complete) were scored in a standard fashion.
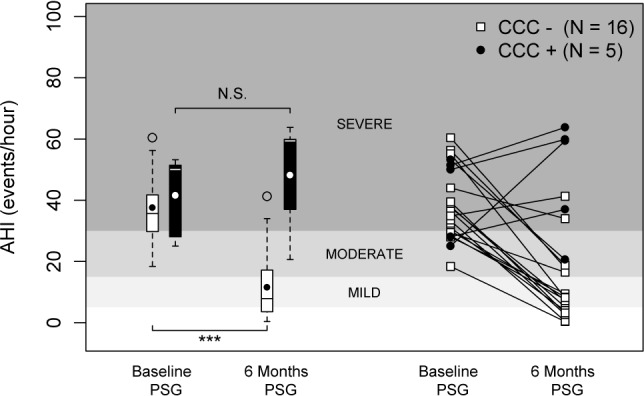
Results: We report on the correlation between DISE results and therapy response in 21 OSA patients (apnea-hypopnea index [AHI] 38.5 ± 11.8/h; body mass index [BMI] 28 ± 2 kg/m(2), age 55 ± 11 y, 20 male/1 female) who underwent DISE before implantation of a UAS system. Statistical analysis revealed a significantly better outcome with UAS in patients (n = 16) without palatal complete concentric collapse (CCC), reducing AHI from 37.6 ± 11.4/h at baseline to 11.1 ± 12.0/h with UAS (p < 0.001). No statistical difference was noted in AHI or BMI at baseline between the patients with and without palatal CCC. In addition, no predictive value was found for the other DISE collapse patterns documented.
Conclusions: The absence of palatal CCC during DISE may predict therapeutic success with implanted UAS therapy. DISE can be recommended as a patient selection tool for implanted UAS to treat OSA.
Keywords: Electrical stimulation; hypoglossal nerve; neuromodulation; obstructive sleep apnea hypopnea syndrome; prediction; sleep disordered breathing; snoring.
Figures
Comment in
-
A prognostic star was born: drug-induced sleep endoscopy for hypoglossal nerve stimulation.J Clin Sleep Med. 2020 Dec 17;16(S1):15-16. doi: 10.5664/jcsm.8882. J Clin Sleep Med. 2020. PMID: 33054960 Free PMC article.
References
-
- Kuna ST, Sant'Ambrogio G. Pathophysiology of upper airway closure during sleep. JAMA. 1991;266:1384–9. - PubMed
-
- Lindberg E, Carter N, Gislason T, Janson C. Role of snoring and daytime sleepiness in occupational accidents. Am J Respir Crit Care Med. 2001;164:2031–5. - PubMed
-
- Kushida CA, Littner MR, Hirshkowitz M, et al. Practice parameters for the use of continuous and bilevel positive airway pressure devices to treat adult patients with sleep-related breathing disorders. Sleep. 2006;29:375–80. - PubMed
-
- Sullivan CE, Issa FG, Berthon-Jones M, Eves L. Reversal of obstructive sleep apnoea by continuous positive airway pressure applied through the nares. Lancet. 1981;1:862–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
