

PD-L1 blockade synergizes with IL-2 therapy in reinvigorating exhausted T cells
- PMID: 23676462
- PMCID: PMC3668811
- DOI: 10.1172/JCI67008
PD-L1 blockade synergizes with IL-2 therapy in reinvigorating exhausted T cells
Abstract
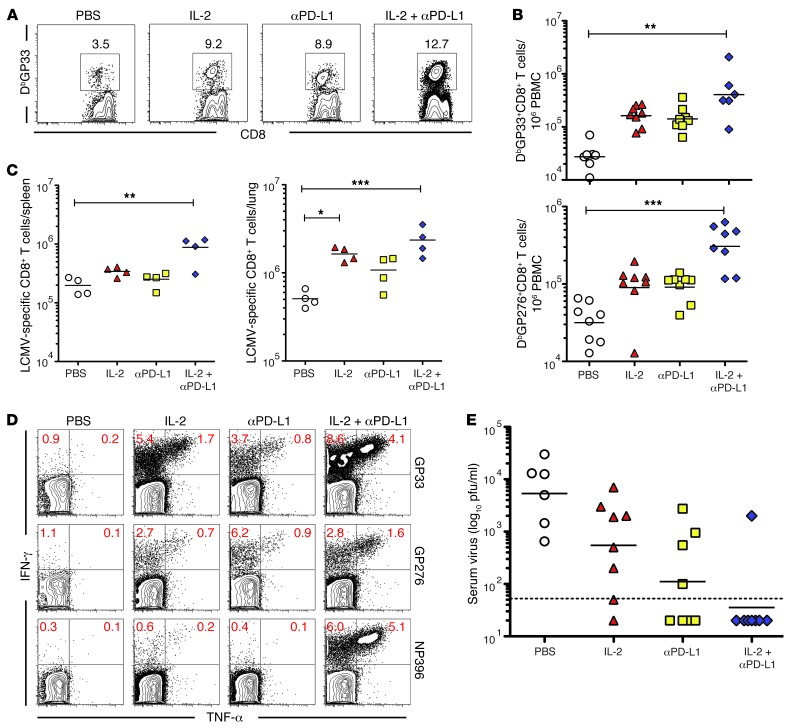
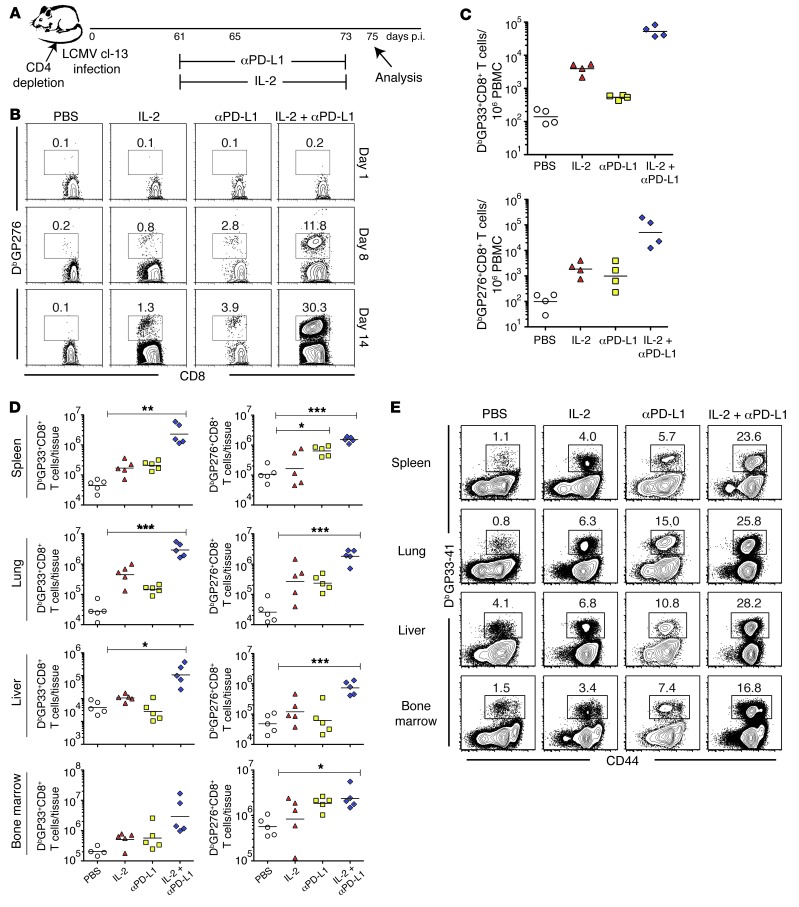
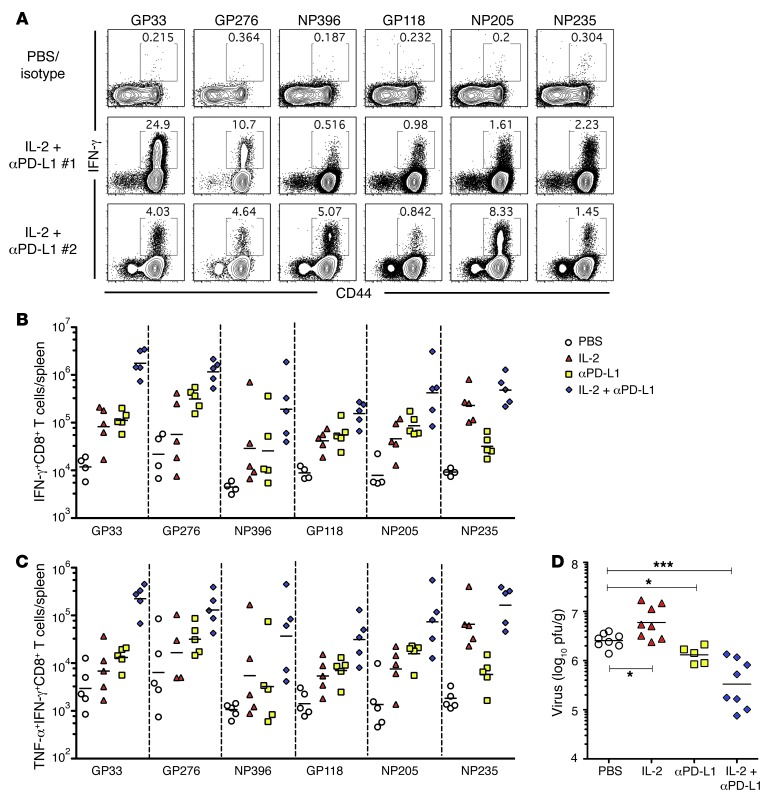
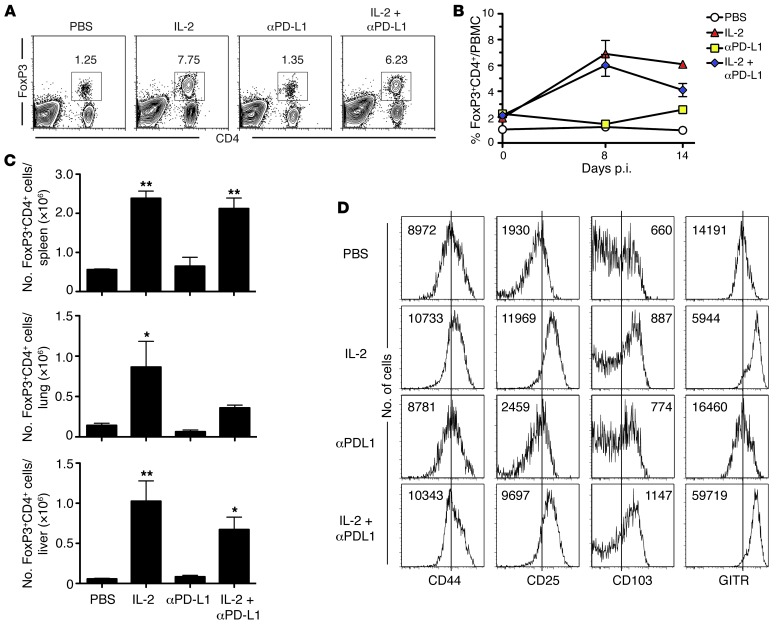
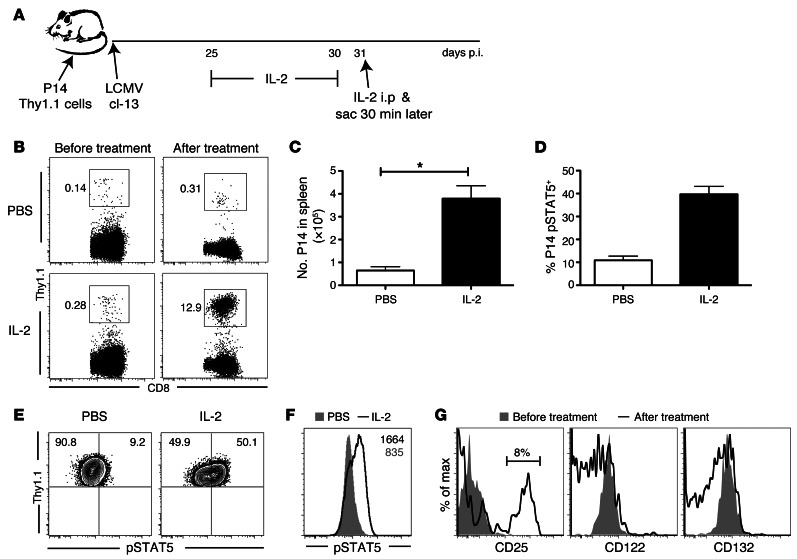
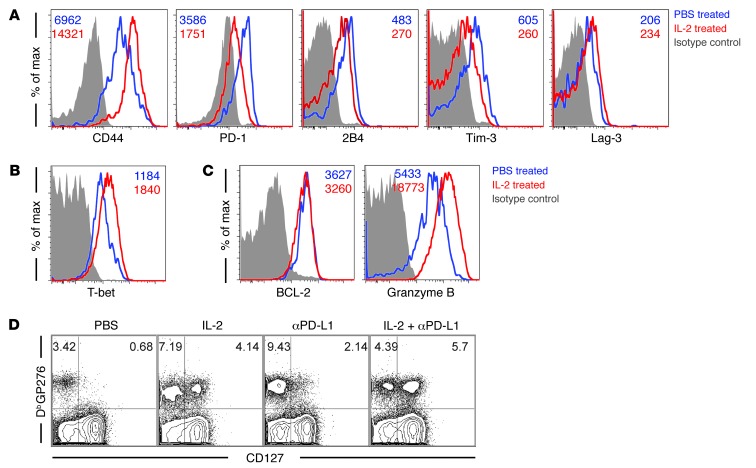
The inhibitory receptor programmed cell death 1 (PD-1) plays a major role in functional exhaustion of T cells during chronic infections and cancer, and recent clinical data suggest that blockade of the PD-1 pathway is an effective immunotherapy in treating certain cancers. Thus, it is important to define combinatorial approaches that increase the efficacy of PD-1 blockade. To address this issue, we examined the effect of IL-2 and PD-1 ligand 1 (PD-L1) blockade in the mouse model of chronic lymphocytic choriomeningitis virus (LCMV) infection. We found that low-dose IL-2 administration alone enhanced CD8+ T cell responses in chronically infected mice. IL-2 treatment also decreased inhibitory receptor levels on virus-specific CD8+ T cells and increased expression of CD127 and CD44, resulting in a phenotype resembling that of memory T cells. Surprisingly, IL-2 therapy had only a minimal effect on reducing viral load. However, combining IL-2 treatment with blockade of the PD-1 inhibitory pathway had striking synergistic effects in enhancing virus-specific CD8+ T cell responses and decreasing viral load. Interestingly, this reduction in viral load occurred despite increased numbers of Tregs. These results suggest that combined IL-2 therapy and PD-L1 blockade merits consideration as a regimen for treating human chronic infections and cancer.
Figures
References
-
- Wherry EJ. T cell exhaustion. Nat Immunol. 2011;12(6):492–499. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
