

Major bleeding events and risk stratification of antithrombotic agents in hemodialysis: results from the DOPPS
- PMID: 23677245
- PMCID: PMC3885984
- DOI: 10.1038/ki.2013.170
Major bleeding events and risk stratification of antithrombotic agents in hemodialysis: results from the DOPPS
Abstract
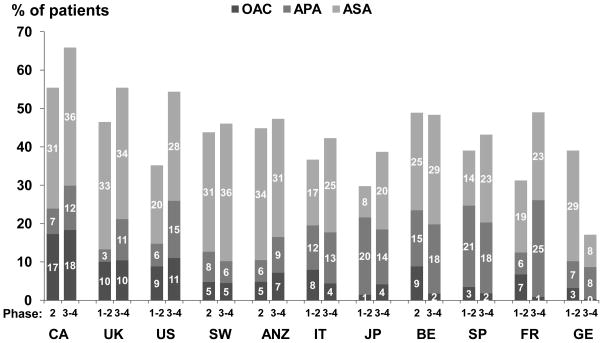
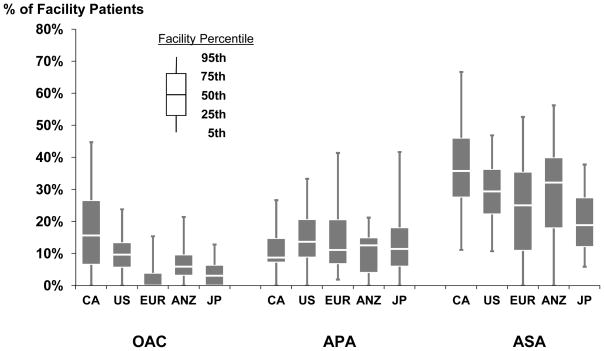
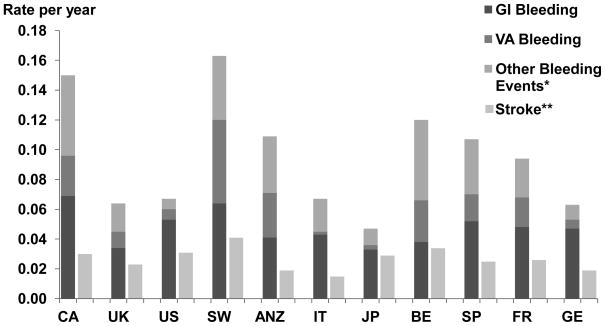
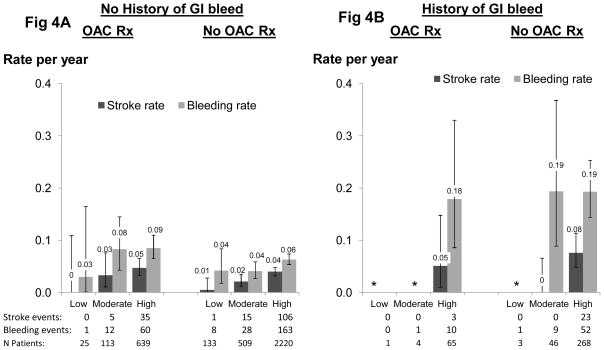
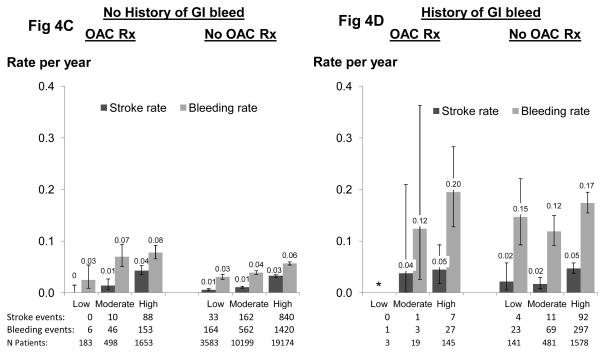
Benefits and risks of antithrombotic agents remain unclear in the hemodialysis population. To help clarify this we determined variation in antithrombotic agent use, rates of major bleeding events, and factors predictive of stroke and bleeding in 48,144 patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS) phases I-IV. Antithrombotic agents including oral anticoagulants (OACs), aspirin (ASA), and anti-platelet agents (APAs) were recorded along with comorbidities at study entry, and clinical events including hospitalization due to bleeding were then collected every 4 months. There was wide variation in OAC (0.3-18%), APA (3-25%), and ASA use (8-36%), and major bleeding rates (0.05-0.22 events/year) among countries. All-cause mortality, cardiovascular mortality, and bleeding events requiring hospitalization were elevated in patients prescribed OACs across adjusted models. The CHADS2 score predicted the risk of stroke in atrial fibrillation patients. Gastrointestinal bleeding in the past 12 months was highly predictive of major bleeding events; for patients with previous gastrointestinal bleeding, the rate of bleeding exceeded the rate of stroke by at least twofold across all categories of CHADS2 score, including patients at high stroke risk. Appropriate risk stratification and a cautious approach should be considered before OAC use in the dialysis population.
Conflict of interest statement
All other authors have no conflicts of interest to report.
Figures
References
-
- Fuster V, Ryden LE, Asinger RW, et al. ACC/AHA/ESC Guidelines for the Management of Patients With Atrial Fibrillation: Executive Summary A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation) Developed in Collaboration With the North American Society of Pacing and Electrophysiology. Circulation. 2001;104:2118–50. - PubMed
-
- Schulman S, Beyth RJ, Kearon C, et al. Hemorrhagic complications of anticoagulant and thrombolytic treatment: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition) Chest. 2008;133:257S–298S. - PubMed
-
- Singer DE, Albers GW, Dalen JE, et al. American College of Chest, Physicians Antithrombotic therapy in atrial fibrillation: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition) Chest. 2008;133:546S–592S. - PubMed
-
- Beyth RJ, Quinn LM, Landefeld CS. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin. Am J Med. 1998;105:91–9. - PubMed
-
- Gage BF, Yan Y, Milligan PE, et al. Clinical classification schemes for predicting hemorrhage: results from the National Registry of Atrial Fibrillation (NRAF) Am Heart J. 2006;151:713–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
