

Long-term outcomes following abdominal sacrocolpopexy for pelvic organ prolapse
- PMID: 23677313
- PMCID: PMC3747840
- DOI: 10.1001/jama.2013.4919
Long-term outcomes following abdominal sacrocolpopexy for pelvic organ prolapse
Erratum in
- JAMA. 2013 Sep 11;310(10):1076
Abstract
Importance: More than 225 000 surgeries are performed annually in the United States for pelvic organ prolapse (POP). Abdominal sacrocolpopexy is considered the most durable POP surgery, but little is known about safety and long-term effectiveness.
Objectives: To describe anatomic and symptomatic outcomes up to 7 years after abdominal sacrocolpopexy, and to determine whether these are affected by concomitant anti-incontinence surgery (Burch urethropexy).
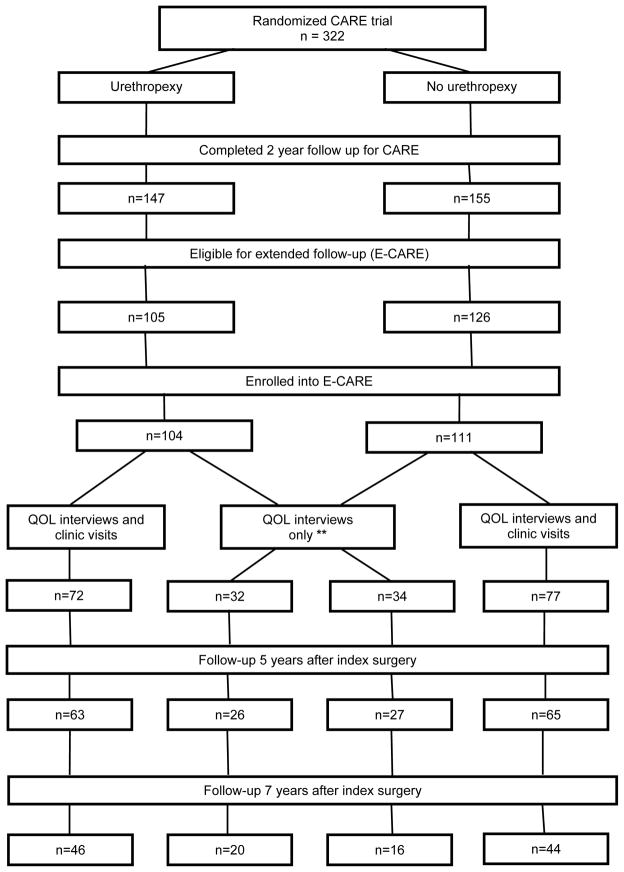
Design, setting, and participants: Long-term follow-up of the randomized, masked 2-year Colpopexy and Urinary Reduction Efforts (CARE) trial of women with stress continence who underwent abdominal sacrocolpopexy between 2002 and 2005 for symptomatic POP and also received either concomitant Burch urethropexy or no urethropexy. Ninety-two percent (215/233) of eligible 2-year CARE trial completers were enrolled in the extended CARE study; and 181 (84%) and 126 (59%) completed 5 and 7 years of follow-up, respectively. The median follow-up was 7 years.
Main outcomes and measures: Symptomatic POP failure requiring retreatment or self-reported bulge; or anatomic POP failure requiring retreatment or Pelvic Organ Prolapse Quantification evaluation demonstrating descent of the vaginal apex below the upper third of the vagina, or anterior or posterior vaginal wall prolapse beyond the hymen. Stress urinary incontinence (SUI) with more than 1 symptom or interval treatment; or overall UI score of 3 or greater on the Incontinence Severity Index.
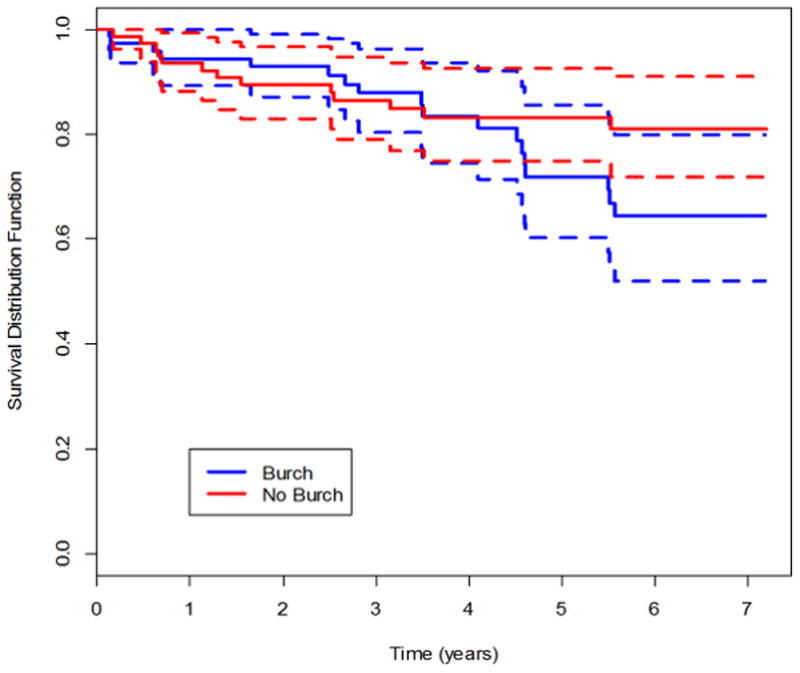
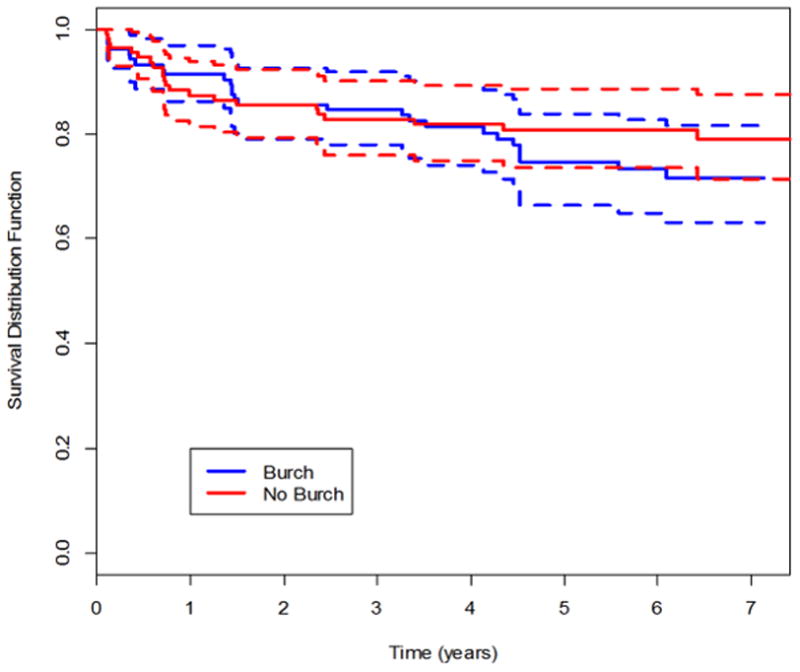
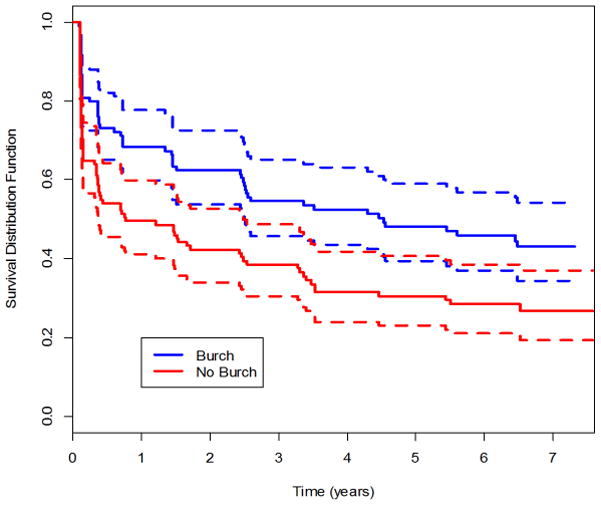
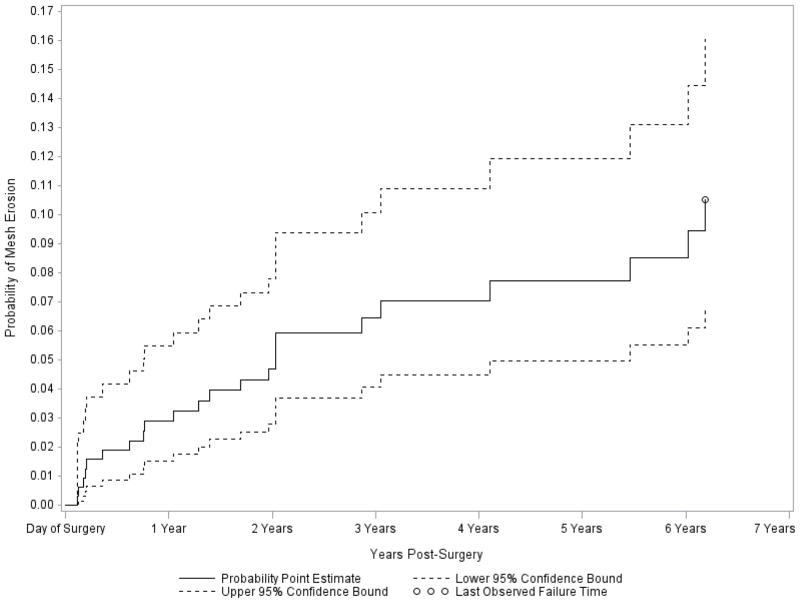
Results: By year 7, the estimated probabilities of treatment failure (POP, SUI, UI) from parametric survival modeling for the urethropexy group and the no urethropexy group, respectively, were 0.27 and 0.22 for anatomic POP (treatment difference of 0.050; 95% CI, -0.161 to 0.271), 0.29 and 0.24 for symptomatic POP (treatment difference of 0.049; 95% CI, -0.060 to 0.162), 0.48 and 0.34 for composite POP (treatment difference of 0.134; 95% CI, -0.096 to 0.322), 0.62 and 0.77 for SUI (treatment difference of -0.153; 95% CI, -0.268 to 0.030), and 0.75 and 0.81 for overall UI (treatment difference of -0.064; 95% CI, -0.161 to 0.032). Mesh erosion probability at 7 years (estimated by the Kaplan-Meier method) was 10.5% (95% CI, 6.8% to 16.1%).
Conclusions and relevance: During 7 years of follow-up, abdominal sacrocolpopexy failure rates increased in both groups. Urethropexy prevented SUI longer than no urethropexy. Abdominal sacrocolpopexy effectiveness should be balanced with long-term risks of mesh or suture erosion.
Trial registration: clinicaltrials.gov Identifier: NCT00099372.
Figures
Comment in
-
Pelvic organ prolapse surgery: long-term outcomes and implications for shared decision making.JAMA. 2013 May 15;309(19):2045-6. doi: 10.1001/jama.2013.5528. JAMA. 2013. PMID: 23677317 No abstract available.
-
Success rates of abdominal sacrocolpopexy decrease over time, but with improved continence rates with concomitant urethropexy.Evid Based Med. 2014 Apr;19(2):55. doi: 10.1136/eb-2013-101461. Epub 2013 Sep 5. Evid Based Med. 2014. PMID: 24009332 No abstract available.
-
Surgery for pelvic organ prolapse.JAMA. 2013 Sep 11;310(10):1073. doi: 10.1001/jama.2013.238041. JAMA. 2013. PMID: 24026605 No abstract available.
-
Surgery for pelvic organ prolapse--reply.JAMA. 2013 Sep 11;310(10):1073-4. doi: 10.1001/jama.2013.238044. JAMA. 2013. PMID: 24026606 No abstract available.
-
Re: long-term outcomes following abdominal sacrocolpopexy for pelvic organ prolapse.J Urol. 2014 Feb;191(2):419. doi: 10.1016/j.juro.2013.10.130. Epub 2013 Nov 1. J Urol. 2014. PMID: 24411877 No abstract available.
References
-
- Olsen AL, Smith VJ, Bergstrom JO, et al. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol. 1997;89:501–506. - PubMed
-
- Smith FJ, Holman CD, Moorin RE, Tsokos N. Lifetime risk of undergoing surgery for pelvic organ prolapse. Obstet Gynecol. 2010;116:1096–100. - PubMed
-
- Nygaard I, McCreery R, Brubaker L, et al. for the Pelvic Floor disorders network. Abdominal Sacrocolpopexy: A Comprehensive Review. Obstet Gynecol. 2004;104:805–23. - PubMed
-
- Subak LL, Waetjen LE, van den Eeden S, Thom DH, Vittinghoff E, Brown JS. Cost of pelvic organ prolapse surgery in the United States. Obstet Gynecol. 2001 Oct;98(4):646–51. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U10 HD041261/HD/NICHD NIH HHS/United States
- U01 HD041249/HD/NICHD NIH HHS/United States
- U10 HD41267/HD/NICHD NIH HHS/United States
- U10 HD054215/HD/NICHD NIH HHS/United States
- U10 HD054214/HD/NICHD NIH HHS/United States
- U10 HD54215/HD/NICHD NIH HHS/United States
- U10 HD41261/HD/NICHD NIH HHS/United States
- U01 HD069031/HD/NICHD NIH HHS/United States
- U10 HD041263/HD/NICHD NIH HHS/United States
- U10 HD041267/HD/NICHD NIH HHS/United States
- U10 HD069006/HD/NICHD NIH HHS/United States
- U10 HD054241/HD/NICHD NIH HHS/United States
- U10 HD041250/HD/NICHD NIH HHS/United States
- U10 HD54241/HD/NICHD NIH HHS/United States
- U10 HD54136/HD/NICHD NIH HHS/United States
- U10 HD41250/HD/NICHD NIH HHS/United States
- U10 HD54214/HD/NICHD NIH HHS/United States
- U01 HD41249/HD/NICHD NIH HHS/United States
- UG1 HD041267/HD/NICHD NIH HHS/United States
- U10 HD054136/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
