

Physical fitness and risk for heart failure and coronary artery disease
- PMID: 23677924
- PMCID: PMC5152944
- DOI: 10.1161/CIRCHEARTFAILURE.112.000054
Physical fitness and risk for heart failure and coronary artery disease
Abstract
Background: Multiple studies have demonstrated strong associations between cardiorespiratory fitness and lower cardiovascular disease mortality. In contrast, little is known about associations of fitness with nonfatal cardiovascular events.
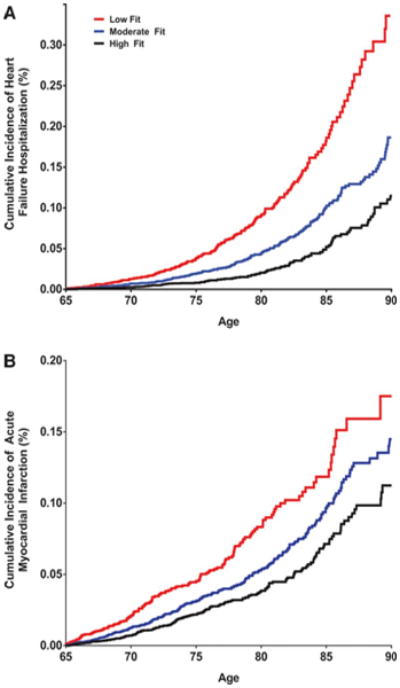
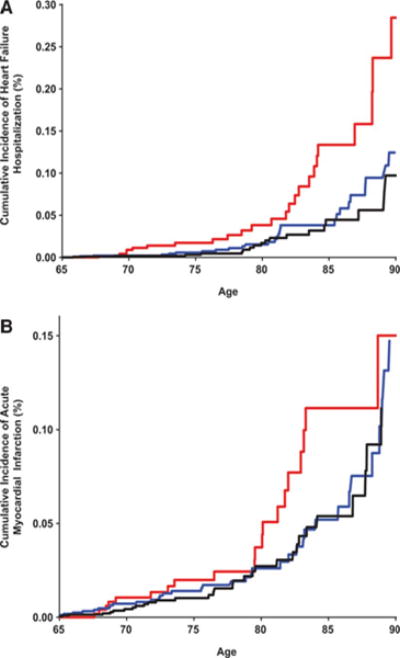
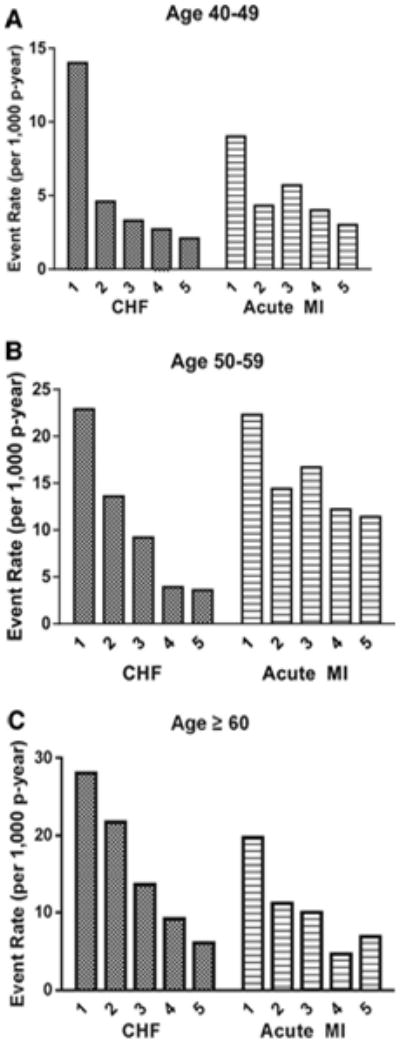
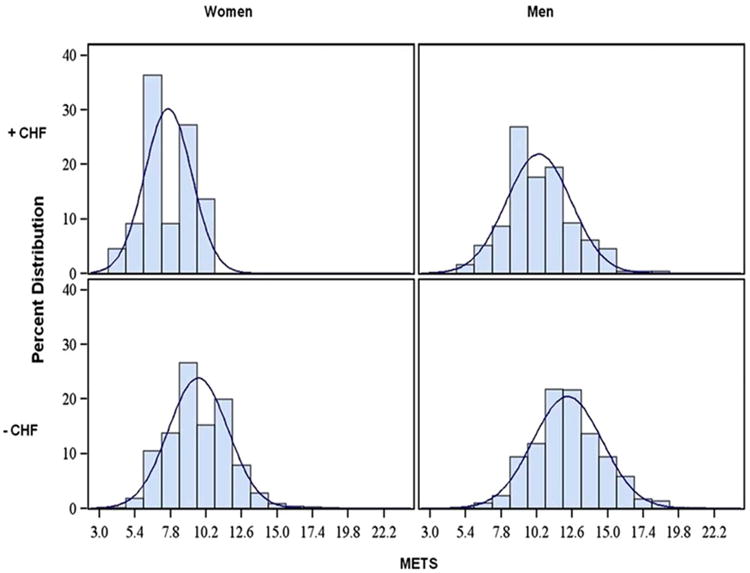
Methods and results: Linking individual participant data from the Cooper Center Longitudinal Study with Medicare claims files, we studied 20642 participants (21% women) with fitness measured at the mean age of 49 years and who survived to receive Medicare coverage from 1999 to 2009. Fitness was categorized into age- and sex-specific quintiles (Q) according to Balke protocol treadmill time with Q1 as low fitness. Fitness was also estimated in metabolic equivalents according to treadmill time. Associations between midlife fitness and hospitalizations for heart failure and acute myocardial infarction after the age of 65 years were assessed by applying a proportional hazards model to the multivariate failure time data. After 133514 person-years of Medicare follow-up, we observed 1051 hospitalizations for heart failure and 832 hospitalizations for acute myocardial infarction. Compared with high fitness (Q4-5), low fitness (Q1) was associated with a higher rate of heart failure hospitalization (14.3% versus 4.2%) and hospitalization for myocardial infarction (9.7% versus 4.5%). After multivariable adjustment for baseline age, blood pressure, diabetes mellitus, body mass index, smoking status, and total cholesterol, a 1 unit greater fitness level in metabolic equivalents achieved in midlife was associated with ≈20% lower risk for heart failure hospitalization after the age of 65 years (men: hazard ratio [95% confidence intervals], 0.79 [0.75-0.83]; P<0.001 and women: 0.81 [0.68-0.96]; P=0.01) but just a 10% lower risk for acute myocardial infarction in men (0.91 [0.87-0.95]; P<0.001) and no association in women (0.97 [0.83-1.13]; P=0.68).
Conclusions: Fitness in healthy, middle-aged adults is more strongly associated with heart failure hospitalization than acute myocardial infarction outcomes decades later in older age.
Figures
References
-
- Paffenbarger RS, Jr, Blair SN, Lee IM, Hyde RT. Measurement of physical activity to assess health effects in free-living populations. Medicine and science in sports and exercise. 1993;25:60–70. - PubMed
-
- Nes BM, Janszky I, Aspenes ST, Bertheussen GF, Vatten LJ, Wisloff U. Exercise patterns and peak oxygen uptake in a healthy population: The hunt study. Medicine and science in sports and exercise. 2012;44:1881–1889. - PubMed
-
- Blair SN, Kohl HW, Barlow CE, Paffenbarger RS, Gibbons LW, Macera CA. Changes in physical fitness and all-cause mortality. A prospective study of healthy and unhealthy men. JAMA. 1995;273:1093–1098. - PubMed
-
- Blair SN, Kohl HW, 3rd, Paffenbarger RS, Jr, Clark DG, Cooper KH, Gibbons LW. Physical fitness and all-cause mortality. A prospective study of healthy men and women. JAMA. 1989;262:2395–2401. - PubMed
-
- Ekelund LG, Haskell WL, Johnson JL, Whaley FS, Criqui MH, Sheps DS. Physical fitness as a predictor of cardiovascular mortality in asymptomatic north american men. The lipid research clinics mortality follow-up study. N Engl J Med. 1988;319:1379–1384. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
