

Evaluation of Xpert MTB/RIF for detection of tuberculosis from blood samples of HIV-infected adults confirms Mycobacterium tuberculosis bacteremia as an indicator of poor prognosis
- PMID: 23678061
- PMCID: PMC3697654
- DOI: 10.1128/JCM.00330-13
Evaluation of Xpert MTB/RIF for detection of tuberculosis from blood samples of HIV-infected adults confirms Mycobacterium tuberculosis bacteremia as an indicator of poor prognosis
Abstract
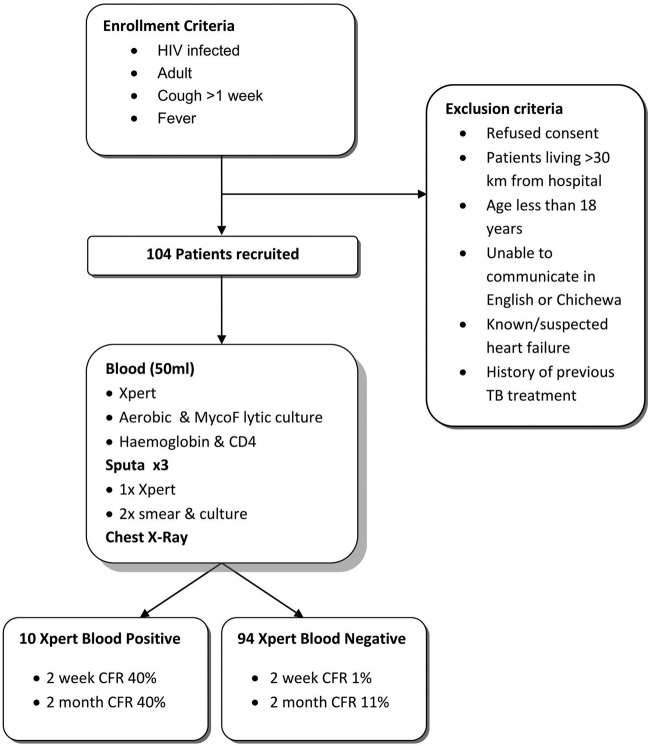
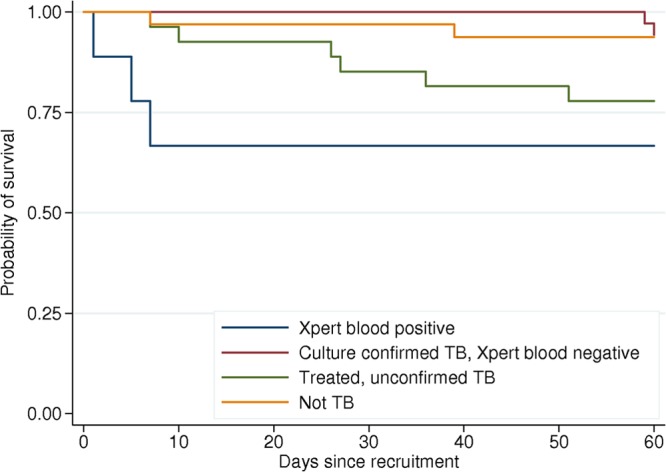
Tuberculosis (TB) remains a leading cause of death among HIV-infected adults, in part because of delayed diagnosis and therefore delayed initiation of treatment. Recently, the Gene-Xpert platform, a rapid, PCR-based diagnostic platform, has been validated for the diagnosis of TB with sputum. We have evaluated the Xpert MTB/RIF assay for the diagnosis of Mycobacterium tuberculosis bacteremia and investigated its impact on clinical outcomes. Consecutive HIV-infected adults with fever and cough presenting to Queen Elizabeth Central Hospital, Blantyre, Malawi, were recruited and followed up for 2 months. At presentation, three sputum samples were examined by smear, culture, and Xpert MTB/RIF assay for the presence of M. tuberculosis and blood was drawn for PCR with Xpert, for mycobacterial culture (Myco/F Lytic), and for aerobic culture. One hundred four patients were recruited, and 44 (43%) were sputum culture positive for M. tuberculosis. Ten were Xpert blood positive, for a sensitivity of 21% and a specificity of 100%. The 2-week mortality rate was significantly higher among patients who were Xpert blood positive than among those who were negative (40% versus 3%; multivariate odds ratio [OR] for death if positive, 44; 95% confidence interval [CI], 3 to 662). This effect persisted on assessment of the mortality rate at 2 months (40% versus 11%; OR, 5.6; 95% CI, 1.3 to 24.6). When screening uncomplicated patients presenting with a productive cough for pulmonary TB, Xpert blood offers no diagnostic advantage over sputum testing. Despite this, Xpert blood positivity is highly predictive of early death and this test rapidly identifies a group of patients in urgent need of initiation of treatment.
Figures
References
-
- Ansari NA, Kombe AH, Kenyon TA, Hone NM, Tappero JW, Nyirenda ST, Binkin NJ, Lucas SB. 2002. Pathology and causes of death in a group of 128 predominantly HIV-positive patients in Botswana, 1997-1998. Int. J. Tuberc. Lung Dis. 6:55–63 - PubMed
-
- Martinson NA, Karstaedt A, Venter WD, Omar T, King P, Mbengo T, Marais E, McIntyre J, Chaisson RE, Hale M. 2007. Causes of death in hospitalized adults with a premortem diagnosis of tuberculosis: an autopsy study. AIDS 21:2043–2050 - PubMed
-
- Rose AG. 1987. Cardiac tuberculosis. A study of 19 patients. Arch. Pathol. Lab. Med. 111:422–426 - PubMed
-
- Archibald LK, den Dulk MO, Pallangyo KJ, Reller LB. 1998. Fatal Mycobacterium tuberculosis bloodstream infections in febrile hospitalized adults in Dar es Salaam, Tanzania. Clin. Infect. Dis. 26:290–296 - PubMed
-
- Archibald LK, McDonald LC, Nwanyanwu O, Kazembe P, Dobbie H, Tokars J, Reller LB, Jarvis WR. 2000. A hospital-based prevalence survey of bloodstream infections in febrile patients in Malawi: implications for diagnosis and therapy. J. Infect. Dis. 181:1414–1420 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
