

Detection of Mycobacterium tuberculosis in blood by use of the Xpert MTB/RIF assay
- PMID: 23678063
- PMCID: PMC3697682
- DOI: 10.1128/JCM.00332-13
Detection of Mycobacterium tuberculosis in blood by use of the Xpert MTB/RIF assay
Abstract
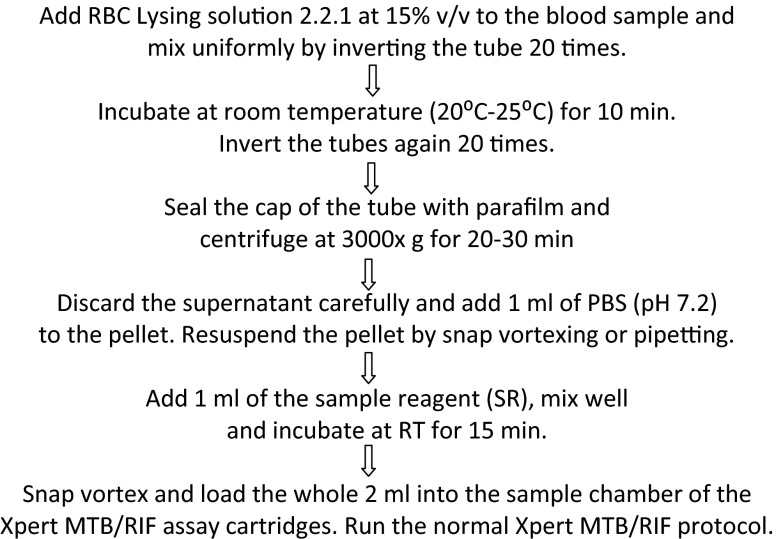
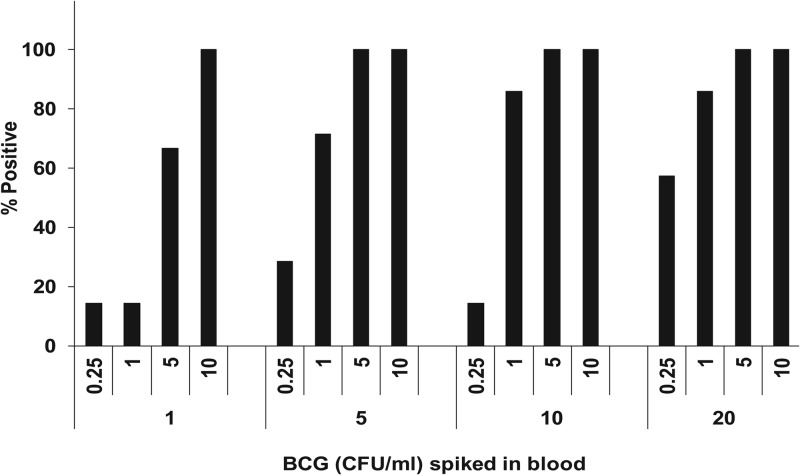
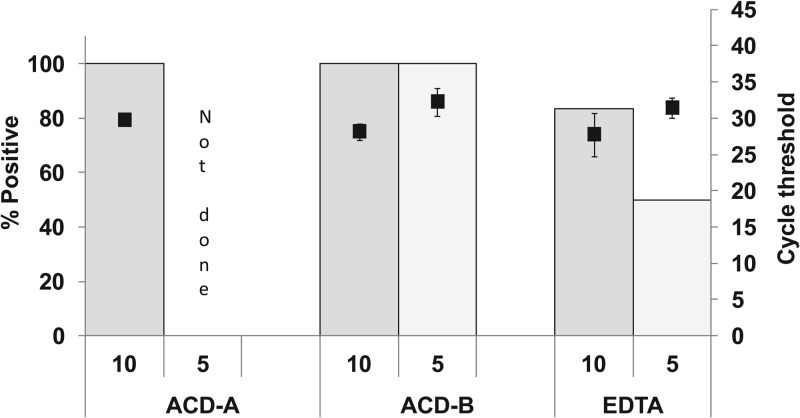
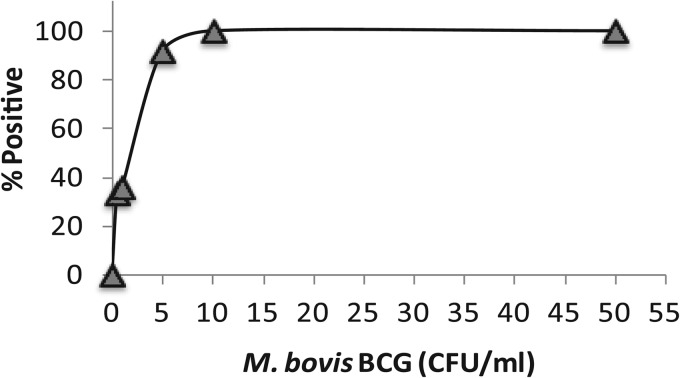
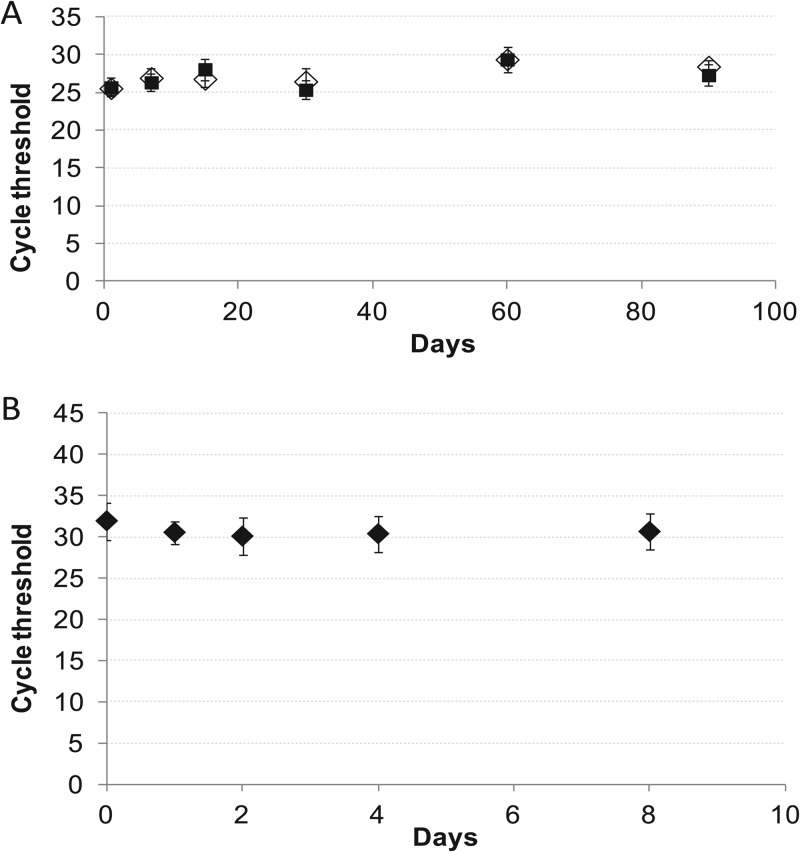
We have developed a novel blood lysis-centrifugation approach for highly sensitive Mycobacterium tuberculosis detection in large volumes of blood with the Xpert MTB/RIF assay. One through 20 ml of blood was spiked with 0.25 to 10 CFU/ml of the M. tuberculosis surrogate M. bovis BCG. Multiple replicates of each sample were processed by a new lysis-centrifugation method and tested with the Xpert MTB/RIF assay. The assay was very sensitive with increased blood volumes. In the 20-ml samples, BCG was detected in blood spiked with 10, 5, 1, and 0.25 CFU/ml 100, 100, 83, and 57% of the time, respectively, compared to 100, 66, 18, and 18%, of the time, respectively, in 1-ml blood samples. Assay sensitivity was influenced by the type of anticoagulant used, with acid-citrate-dextrose solution B (ACD-B) providing the best results. A limit of detection of 10 CFU/ml was established with BCG spiked into ACD-B-treated blood, and 92, 36, and 33% of the samples with 5, 1, and 0.5 CFU/ml, respectively, were assay positive. The lysis buffer was stable both at room temperature and at 4°C for 2 months. The assay was tested with blood stored for 8 days without a change in sensitivity as measured by cycle threshold. This new assay format extends the capability of the Xpert MTB/RIF test, enabling up to 20 ml of blood to be tested rapidly for the presence of M. tuberculosis. This approach may be a useful method to detect extrapulmonary tuberculosis and the risk of death in immunocompromised patients.
Figures
References
-
- Gandhi NR, Moll A, Sturm AW, Pawinski R, Govender T, Lalloo U, Zeller K, Andrews J, Friedland G. 2006. Extensively drug-resistant tuberculosis as a cause of death in patients co-infected with tuberculosis and HIV in a rural area of South Africa. Lancet 368:1575–1580 - PubMed
-
- Golden MP, Vikram HR. 2005. Extrapulmonary tuberculosis: an overview. Am. Fam. Physician 72:1761–1768 - PubMed
-
- Peto HM, Pratt RH, Harrington TA, LoBue PA, Armstrong LR. 2009. Epidemiology of extrapulmonary tuberculosis in the United States, 1993-2006. Clin. Infect. Dis. 49:1350–1357 - PubMed
-
- von Reyn CF. 1999. The significance of bacteremic tuberculosis among persons with HIV infection in developing countries. AIDS 13:2193–2195 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
