

Comparison of cytomegalovirus (CMV) enzyme-linked immunosorbent spot and CMV quantiferon gamma interferon-releasing assays in assessing risk of CMV infection in kidney transplant recipients
- PMID: 23678073
- PMCID: PMC3719636
- DOI: 10.1128/JCM.00563-13
Comparison of cytomegalovirus (CMV) enzyme-linked immunosorbent spot and CMV quantiferon gamma interferon-releasing assays in assessing risk of CMV infection in kidney transplant recipients
Erratum in
- J Clin Microbiol. 2014 Mar;52(3):1025
Abstract
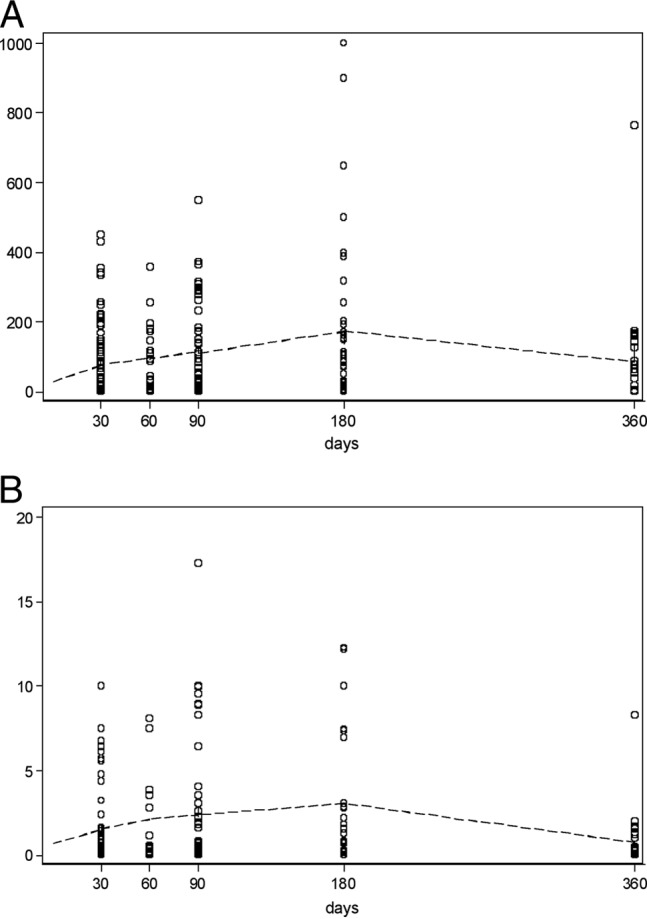
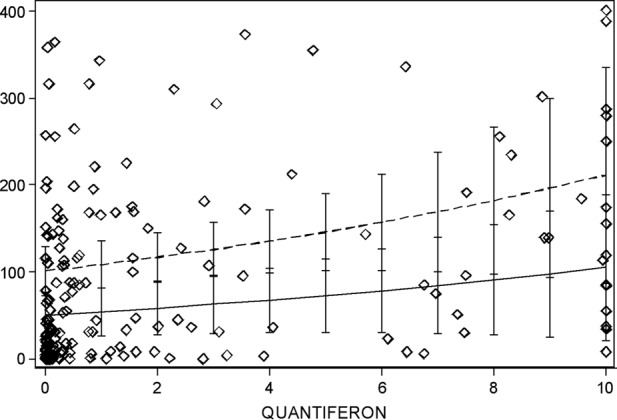
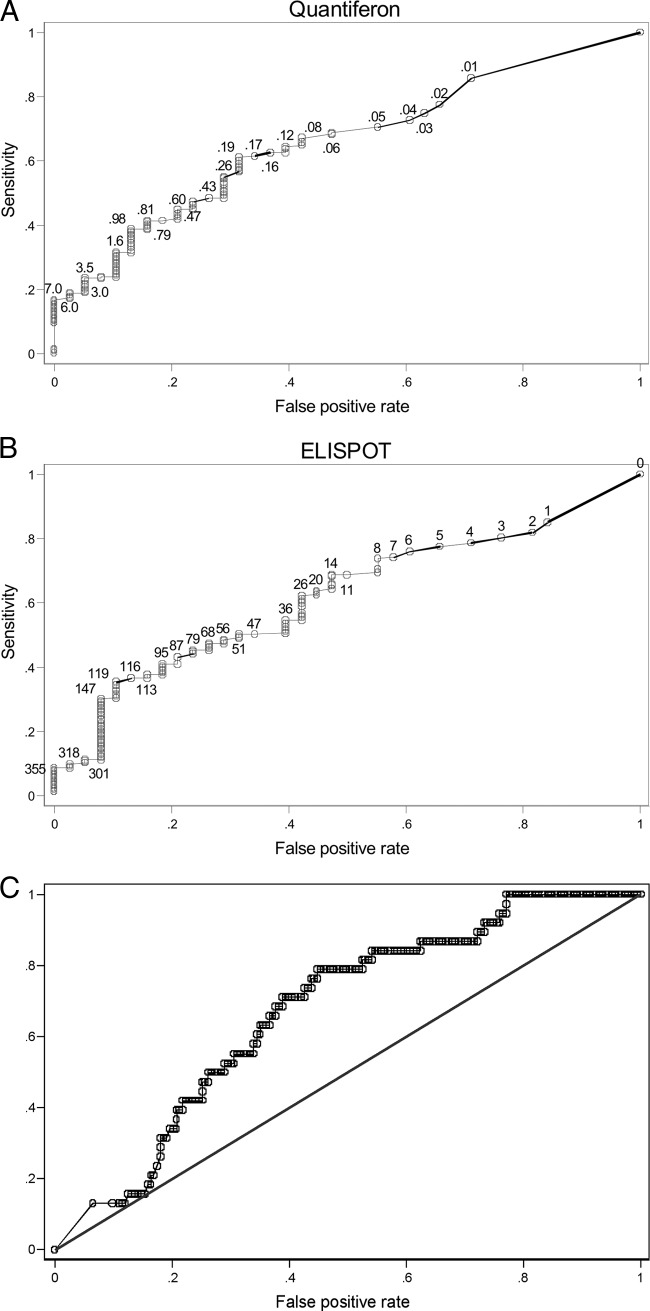
Assessing cytomegalovirus (CMV)-specific cell-mediated immunity (CMI) represents an appealing strategy for identifying transplant recipients at risk of infection. In this study, we compared two gamma interferon-releasing assays (IGRAs), Quantiferon-CMV and CMV enzyme-linked immunosorbent spot (ELISPOT), to determine the ability of each test to predict protective CMV-specific T-cell responses. Two hundred twenty-one Quantiferon-CMV and ELISPOT tests were conducted on 120 adult kidney transplant recipients (KTRs), including 100 CMV-seropositive transplant recipients (R+) and 20 CMV-seronegative transplant recipients of a CMV-positive donor (D+/R-). As a control cohort, 39 healthy adult subjects (including 33 CMV-seropositive and 6 CMV-seronegative subjects) were enrolled. CMV IgG serology was used as a reference for both tests. In the CMV-seropositive individuals, the ELISPOT and Quantiferon-CMV assays provided 46% concordance with the serology, 12% discordance, 18% disagreement between ELISPOT or Quantiferon-CMV and the serology, and 24% gray areas when one or both tests resulted in weak positives. None of the CMV-seronegative subjects showed detectable responses in the ELISPOT or the Quantiferon-CMV test. In transplant recipients, both the ELISPOT and Quantiferon-CMV assays positively correlated with each other and negatively correlated with CMV DNAemia in a significant way (P<0.05). During the antiviral prophylaxis, all 20 D+/R- KTRs we examined displayed undetectable Quantiferon-CMV and ELISPOT results, and there was no evidence of CMV seroconversion. The receiving operator curve (ROC) statistical analysis revealed similar specificities and sensitivities in predicting detectable viremia (areas under the curve [AUC], 0.66 and 0.62 for Quantiferon-CMV and ELISPOT, respectively). ELISPOT and Quantiferon-CMV values of >150 spots/200,000 peripheral blood mononuclear cells (PBMCs) and >1 to 6 IU gamma interferon (IFN-γ) were associated with protection from CMV infection (odds ratios [OR], 5 and 8.75, respectively). In transplant recipients, the two tests displayed similar abilities for predicting CMV infection. Both the ELISPOT and Quantiferon-CMV assays require several ameliorations to avoid false-negative results.
Figures
References
-
- Danziger-Isakov L, Heeger PS. 2009. Clinical utility of measuring T-cell immunity to CMV in transplant recipients. Am. J. Transplant. 9:987–988 - PubMed
-
- Gerna G, Lilleri D. 2006. Monitoring transplant patients for human cytomegalovirus: diagnostic update. Herpes 13:4–11 - PubMed
-
- Kotton CN. 2013. CMV: prevention, diagnosis and therapy. Am. J. Transplant. 13(Suppl. 3):24–40 - PubMed
-
- Nebbia G, Mattes FM, Smith C, Hainsworth E, Kopycinski J, Burroughs A, Griffiths PD, Klenerman P, Emery VC. 2008. Polyfunctional cytomegalovirus-specific CD4+ and pp65 CD8+ T cells protect against high-level replication after liver transplantation. Am. J. Transplant. 8:2590–2599 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
