

Surrogate endpoints for overall survival in chemotherapy and radiotherapy trials in operable and locally advanced lung cancer: a re-analysis of meta-analyses of individual patients' data
- PMID: 23680111
- PMCID: PMC3732017
- DOI: 10.1016/S1470-2045(13)70158-X
Surrogate endpoints for overall survival in chemotherapy and radiotherapy trials in operable and locally advanced lung cancer: a re-analysis of meta-analyses of individual patients' data
Abstract
Background: The gold standard endpoint in clinical trials of chemotherapy and radiotherapy for lung cancer is overall survival. Although reliable and simple to measure, this endpoint takes years to observe. Surrogate endpoints that would enable earlier assessments of treatment effects would be useful. We assessed the correlations between potential surrogate endpoints and overall survival at individual and trial levels.
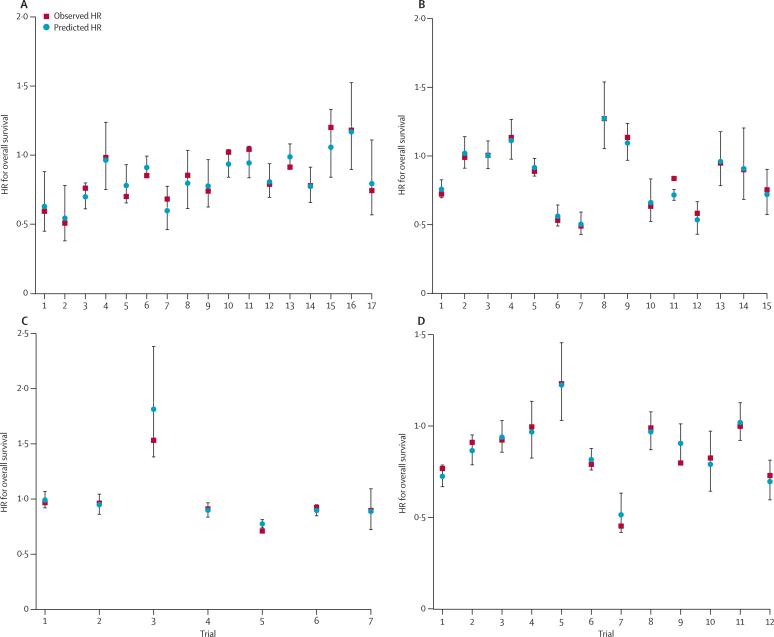
Methods: We analysed individual patients' data from 15,071 patients involved in 60 randomised clinical trials that were assessed in six meta-analyses. Two meta-analyses were of adjuvant chemotherapy in non-small-cell lung cancer, three were of sequential or concurrent chemotherapy, and one was of modified radiotherapy in locally advanced lung cancer. We investigated disease-free survival (DFS) or progression-free survival (PFS), defined as the time from randomisation to local or distant relapse or death, and locoregional control, defined as the time to the first local event, as potential surrogate endpoints. At the individual level we calculated the squared correlations between distributions of these three endpoints and overall survival, and at the trial level we calculated the squared correlation between treatment effects for endpoints.
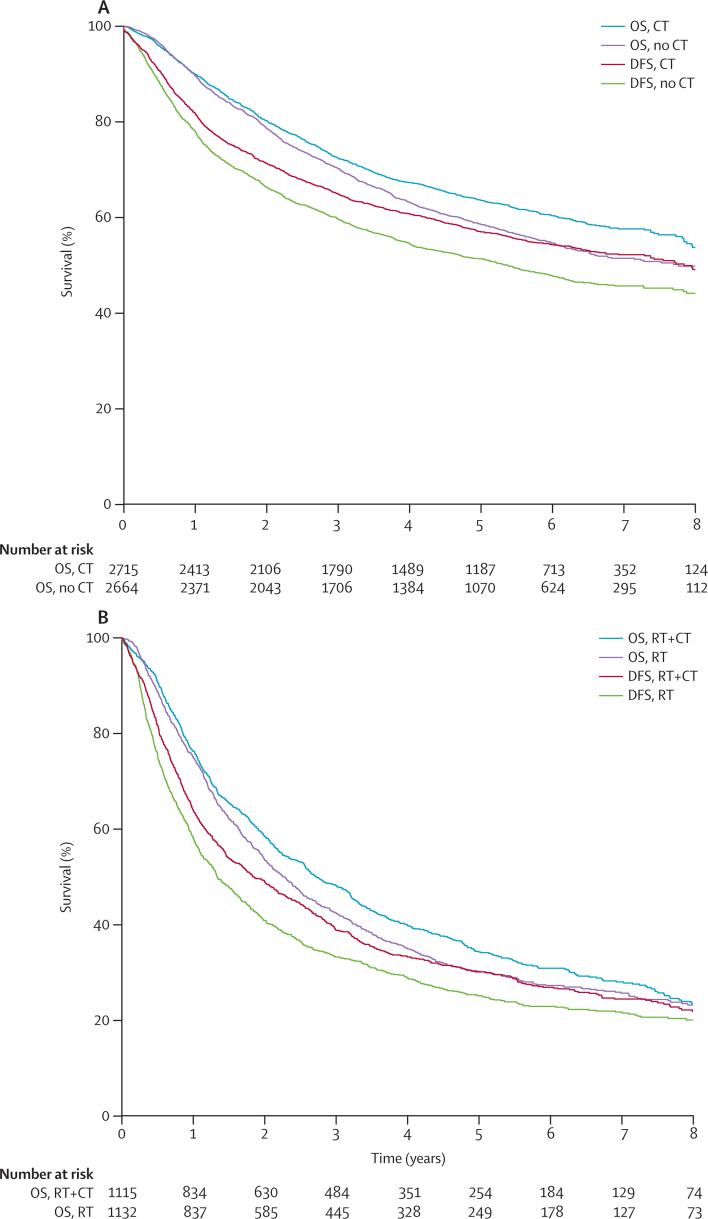
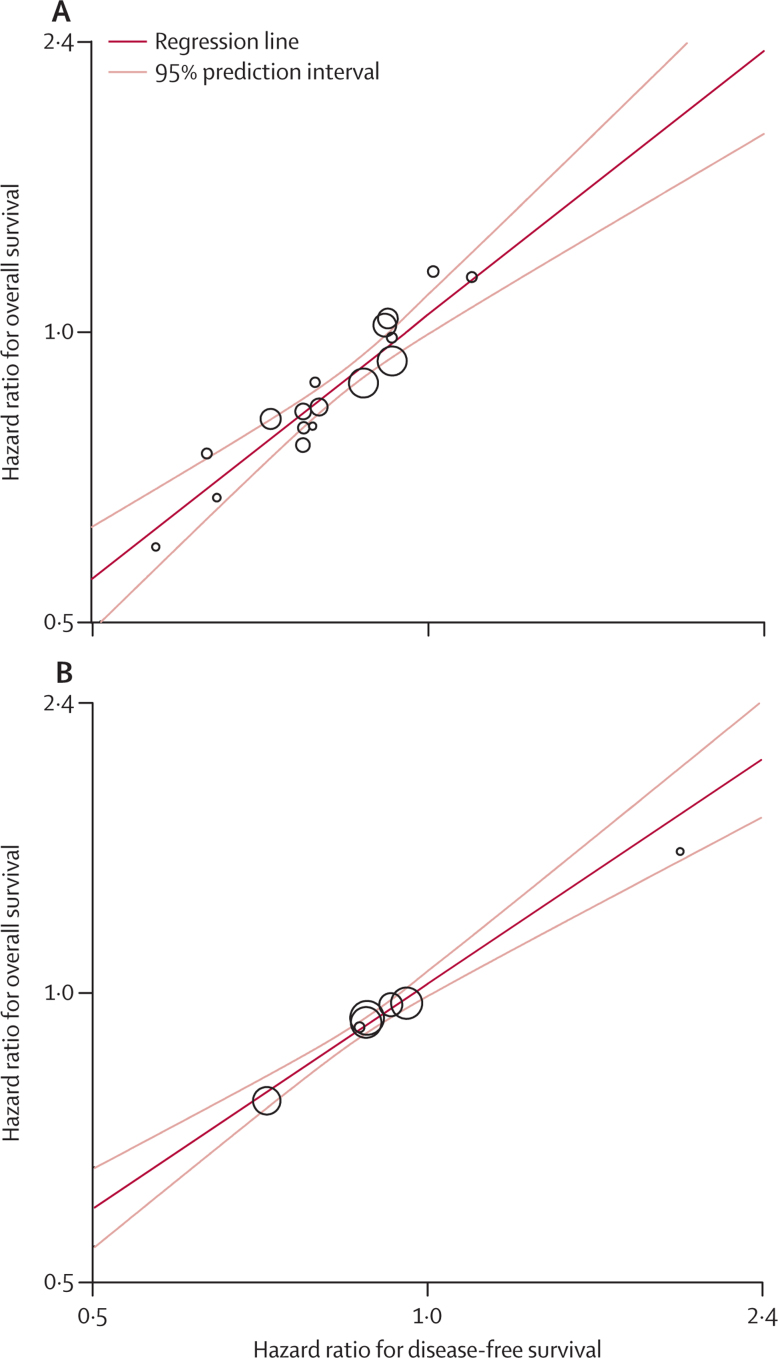
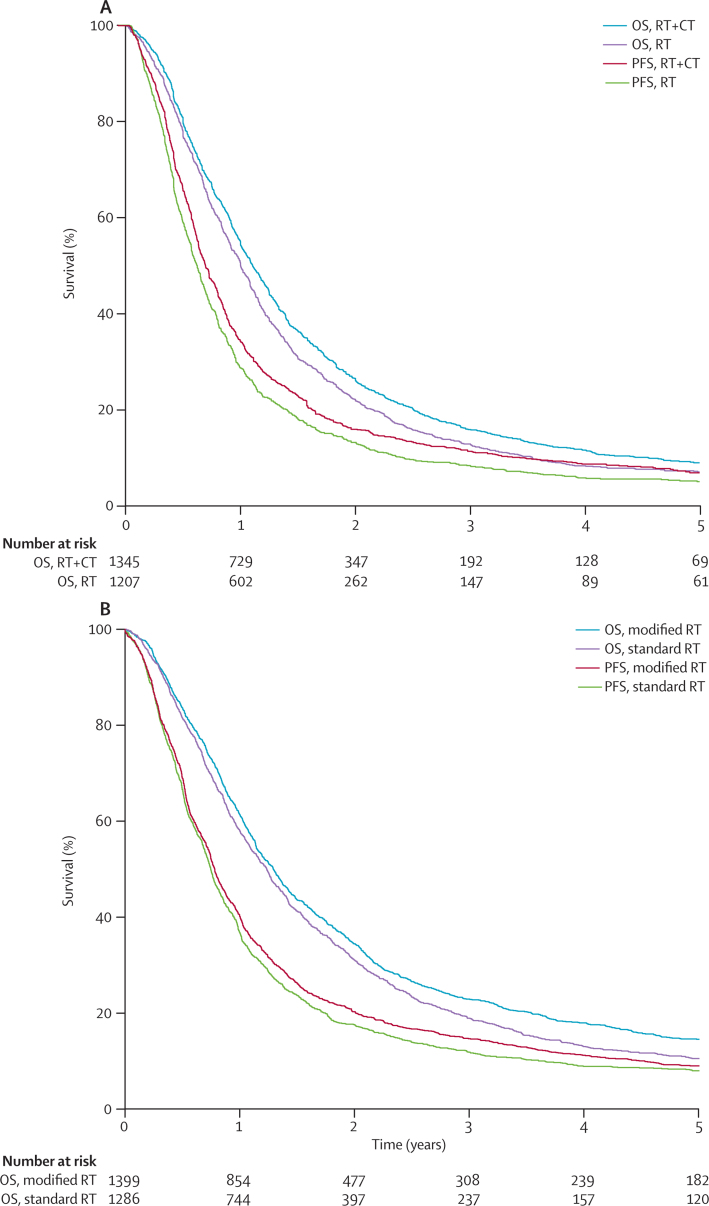
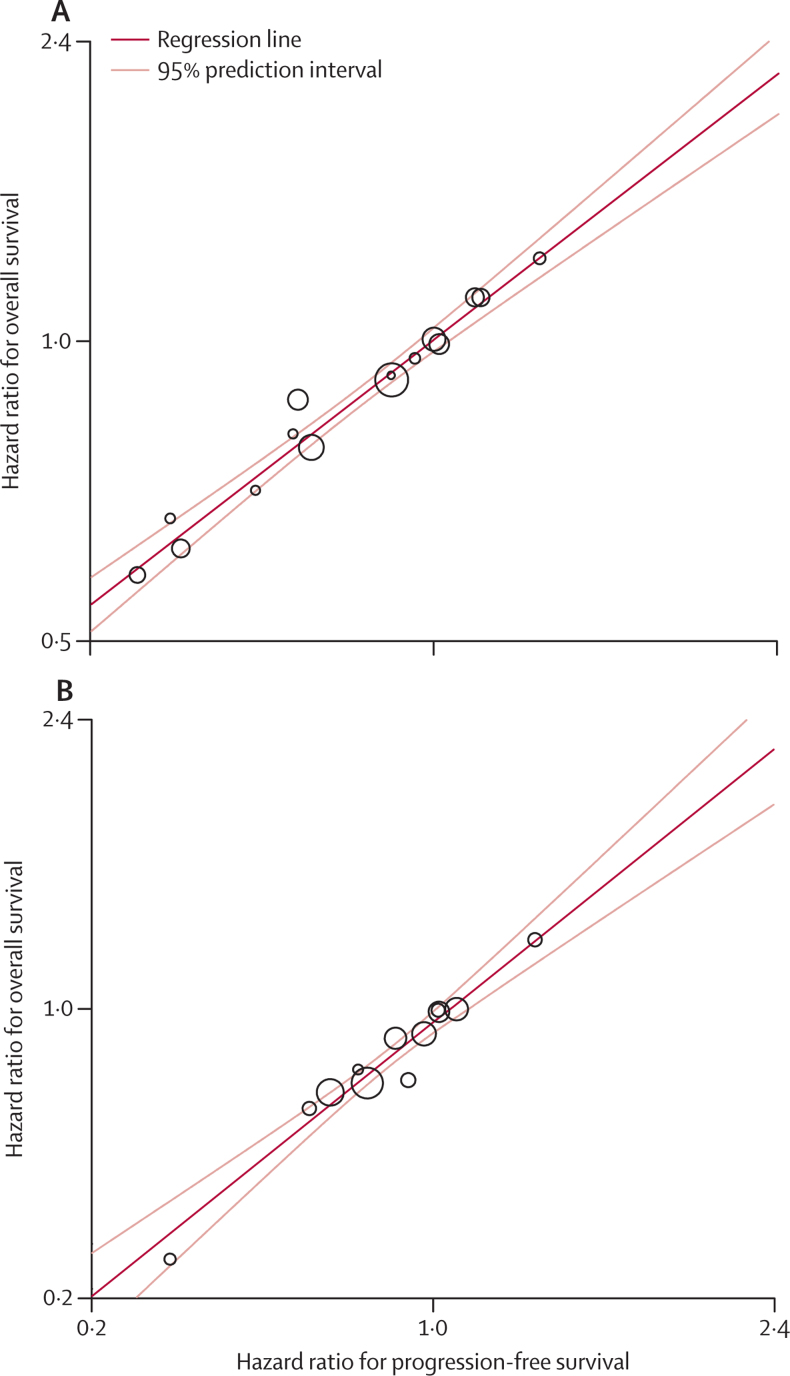
Findings: In trials of adjuvant chemotherapy, correlations between DFS and overall survival were very good at the individual level (ρ(2)=0.83, 95% CI 0.83-0.83 in trials without radiotherapy, and 0.87, 0.87-0.87 in trials with radiotherapy) and excellent at trial level (R(2)=0.92, 95% CI 0.88-0.95 in trials without radiotherapy and 0.99, 0.98-1.00 in trials with radiotherapy). In studies of locally advanced disease, correlations between PFS and overall survival were very good at the individual level (ρ(2) range 0.77-0.85, dependent on the regimen being assessed) and trial level (R(2) range 0.89-0.97). In studies with data on locoregional control, individual-level correlations were good (ρ(2)=0.71, 95% CI 0.71-0.71 for concurrent chemotherapy and ρ(2)=0.61, 0.61-0.61 for modified vs standard radiotherapy) and trial-level correlations very good (R(2)=0.85, 95% CI 0.77-0.92 for concurrent chemotherapy and R(2)=0.95, 0.91-0.98 for modified vs standard radiotherapy).
Interpretation: We found a high level of evidence that DFS is a valid surrogate endpoint for overall survival in studies of adjuvant chemotherapy involving patients with non-small-cell lung cancers, and PFS in those of chemotherapy and radiotherapy for patients with locally advanced lung cancers. Extrapolation to targeted agents, however, is not automatically warranted.
Funding: Programme Hospitalier de Recherche Clinique, Ligue Nationale Contre le Cancer, British Medical Research Council, Sanofi-Aventis.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Surrogate endpoints: can size of effect mitigate perplexity?Lancet Oncol. 2013 Jun;14(7):568-9. doi: 10.1016/S1470-2045(13)70196-7. Epub 2013 May 14. Lancet Oncol. 2013. PMID: 23680110 No abstract available.
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- D'Addario G, Fruh M, Reck M. Metastatic non-small-cell lung cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2010;21(suppl 5):v116–v119. - PubMed
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Little AG, Rusch VW, Bonner JA. Patterns of surgical care of lung cancer patients. Ann Thorac Surg. 2005;80:2051–2056. - PubMed
-
- Johnson JR, Ning YM, Farrell A, Justice R, Keegan P, Pazdur R. Accelerated approval of oncology products: the food and drug administration experience. J Natl Cancer Inst. 2011;103:636–644. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
