

Ultra-early tranexamic acid after subarachnoid hemorrhage (ULTRA): study protocol for a randomized controlled trial
- PMID: 23680226
- PMCID: PMC3658919
- DOI: 10.1186/1745-6215-14-143
Ultra-early tranexamic acid after subarachnoid hemorrhage (ULTRA): study protocol for a randomized controlled trial
Abstract
Background: A frequent complication in patients with subarachnoid hemorrhage (SAH) is recurrent bleeding from the aneurysm. The risk is highest within the first 6 hours after the initial hemorrhage. Securing the aneurysm within this timeframe is difficult owing to logistical delays. The rate of recurrent bleeding can also be reduced by ultra-early administration of antifibrinolytics, which probably improves functional outcome. The aim of this study is to investigate whether ultra-early and short-term administration of the antifibrinolytic agent tranexamic acid (TXA), as add-on to standard SAH management, leads to better functional outcome.
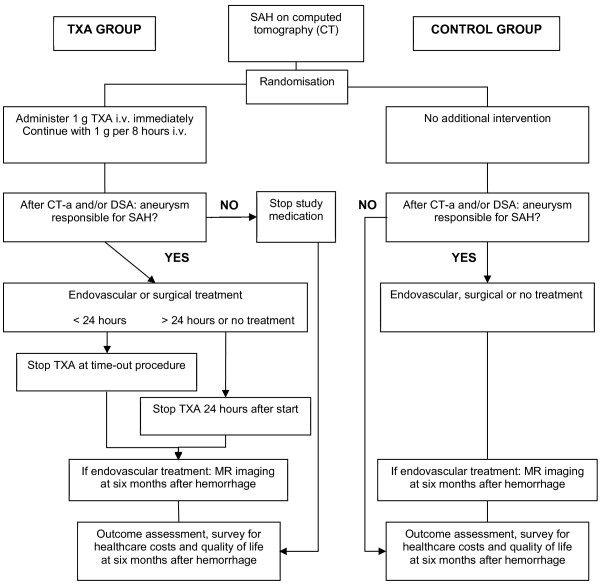
Methods/design: This is a multicenter, prospective, randomized, open-label trial with blinded endpoint (PROBE) assessment. Adult patients with the diagnosis of non-traumatic SAH, as proven by computed tomography (CT) within 24 hours after the onset of headache, will be randomly assigned to the treatment group or the control group. Patients in the treatment group will receive standard treatment with the addition of a bolus of TXA (1 g intravenously) immediately after randomization, followed by continuous infusion of 1 g per 8 hours until the start of aneurysm treatment, or a maximum of 24 hours after the start of medication. Patients in the control group will receive standard treatment without TXA. The primary outcome measure is favorable functional outcome, defined as a score of 0 to 3 on the modified Rankin Scale (mRS), at 6 months after SAH. Primary outcome will be determined by a trial nurse blinded for treatment allocation. We aim to include 950 patients in 3 years.
Discussion: The strengths of this study are: 1. the ultra-early and short-term administration of TXA, resulting in a lower dose as compared to previous studies, which should reduce the risk for delayed cerebral ischemia (DCI), an important risk factor in the long-term treatment with antifibrinolytics; 2. the power calculation is based on functional outcome and calculated with use of recent study results of our own population, supported by data from prominent studies; and 3. the participation of several specialized SAH centers, and their referring hospitals, in the Netherlands with comparative treatment protocols.
Trial registration: Nederlands Trial Register (Dutch Trial Registry) number NTR3272.
References
-
- Wermer MJ, Kool H, Albrecht KW, Rinkel GJ. Subarachnoid hemorrhage treated with clipping: long-term effects on employment, relationships, personality, and mood. Neurosurgery. 2007;60:91–97. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
