

Indocyanine green angiography in posterior uveitis
- PMID: 23685486
- PMCID: PMC3714951
- DOI: 10.4103/0301-4738.112159
Indocyanine green angiography in posterior uveitis
Abstract
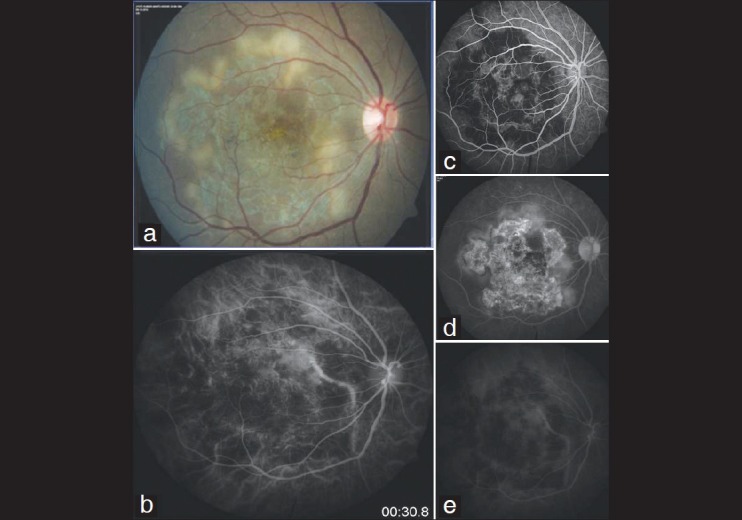
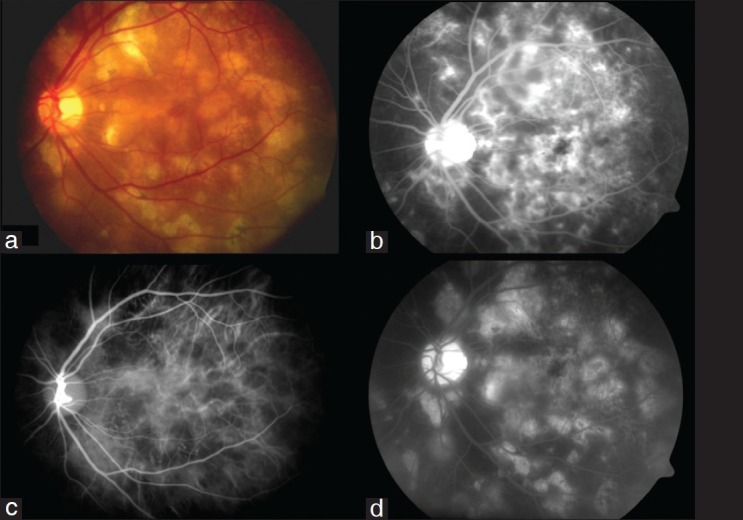
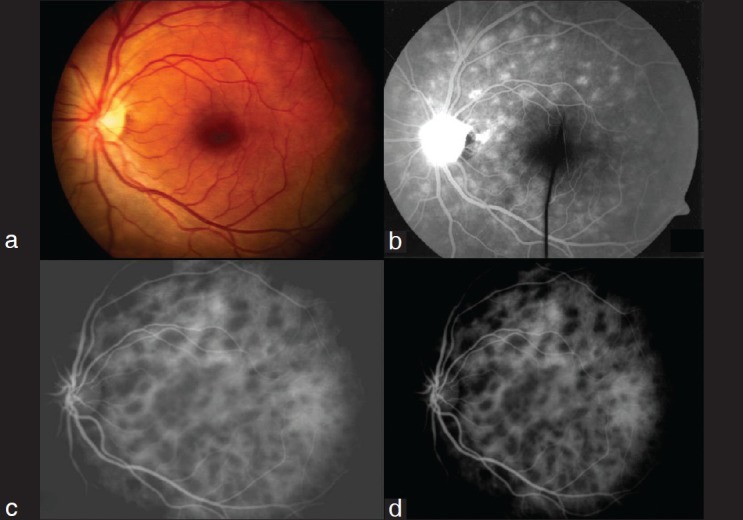
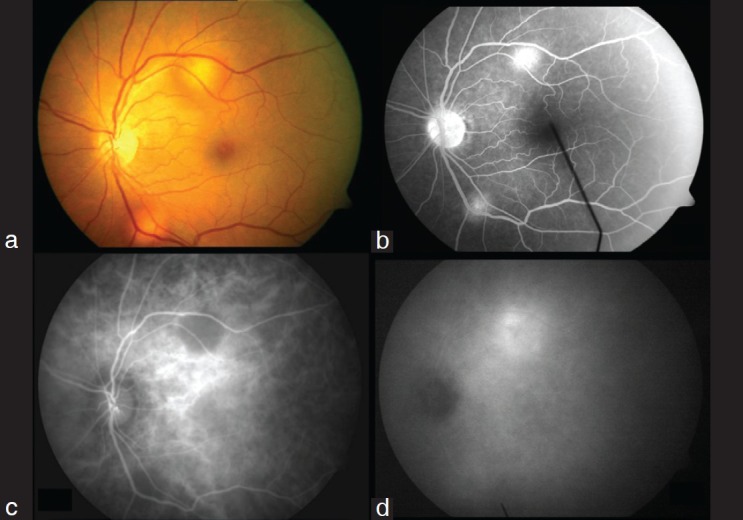
Literature review for indocyanine green angiography and evaluate the role of indocyanine green angiogram (ICGA) in patients with posterior uveitis seen at a tertiary referral eye care centre. Detailed review of the literature on ICGA was performed. Retrospective review of medical records of patients with posterior uveitis and dual fundus and ICGA was done after institutional board approval. Eighteen patients (26 eyes) had serpiginous choroiditis out of which 12 patients had active choroiditis and six patients had healed choroiditis, six patients (12 eyes) had ampiginous choroiditis, six patients (12 eyes) had acute multifocal posterior placoid pigment epitheliopathy, eight patients (10 eyes) had multifocal choroiditis, four patients (eight eyes) had presumed ocular histoplasmosis syndrome, four patients (eight eyes) had presumed tuberculous choroiditis, two patients (four eyes) had multiple evanescent white dot syndrome and two patients (four eyes) had Vogt Koyanagi Harada (VKH) syndrome. The most characteristic feature noted on ICGA was the presence of different patterns of hypofluorescent dark spots, which were present at different stages of the angiogram. ICGA provides the clinician with a powerful adjunctive tool in choroidal inflammatory disorders. It is not meant to replace already proven modalities such as the fluorescein angiography, but it can provide additional information that is useful in establishing a more definitive diagnosis in inflammatory chorioretinal diseases associated with multiple spots. It still needs to be determined if ICGA can prove to be a follow up parameter to evaluate disease progression.
Conflict of interest statement
Figures
Comment in
-
Imaging in vitreoretinal diagnostics.Indian J Ophthalmol. 2013 Apr;61(4):145-7. doi: 10.4103/0301-4738.112158. Indian J Ophthalmol. 2013. PMID: 23685485 Free PMC article. No abstract available.
References
-
- Streilein JW. Ocular immune privilege: Therapeutic opportunities from an experiment of nature. Nat Rev Immunol. 2003;3:879–89. - PubMed
-
- Listhaus AD, Freeman WR. Fluorescein angiography in patients with posterior uveitis. Int Ophthalmol Clin. 1990;30:297–308. - PubMed
-
- Herbort CP, Bodaghi B, Lehoang P. Indocyanine green angiography in ocular inflammatory diseases: Principles, schematic interpretation, semiology and clinical value. J Fr Ophtalmol. 2001;24:423–47. - PubMed
-
- Flower RW, Hochheimer BF. A clinical technique and apparatus for simultaneous angiography of the separate retinal and choroidal circulations. Invest Ophthalmol. 1973;12:248–61. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
