

A case series of primary central nervous system posttransplantation lymphoproliferative disorder: imaging and clinical characteristics
- PMID: 23685504
- PMCID: PMC4442016
- DOI: 10.1227/NEU.0b013e31828cf619
A case series of primary central nervous system posttransplantation lymphoproliferative disorder: imaging and clinical characteristics
Abstract
Background: Primary central nervous system posttransplantation lymphoproliferative disorder (PCNS-PTLD) is a rare complication after solid organ transplantation (SOT). With increasing rates of SOT, PCNS-PTLD incidence is increasing.
Objective: To describe the characteristics of PCNS-PTLD patients requiring neurosurgical intervention.
Methods: From 2000 to 2011, 10 patients with prior SOT underwent biopsy for evaluation of brain lesions and were diagnosed with PCNS-PTLD. Data collected included imaging characteristics, pathology, treatments administered, and survival outcomes.
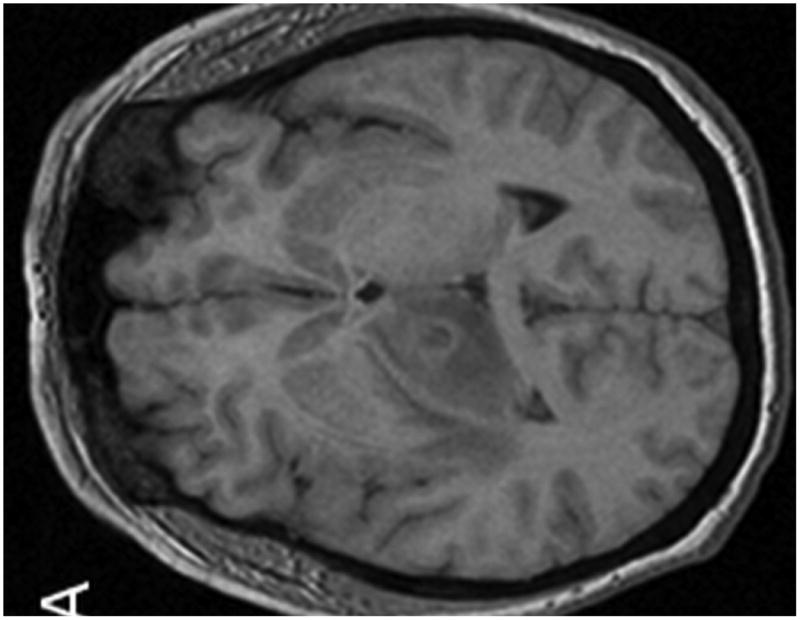
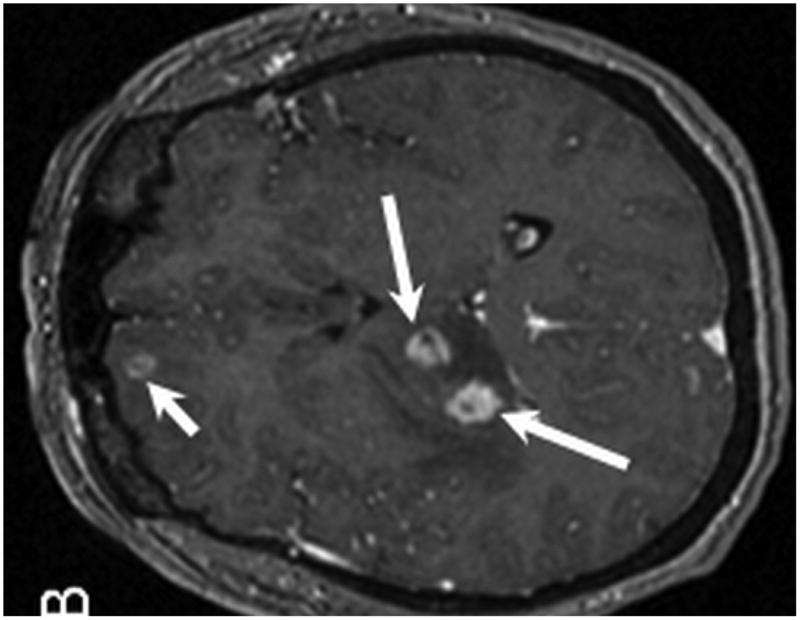
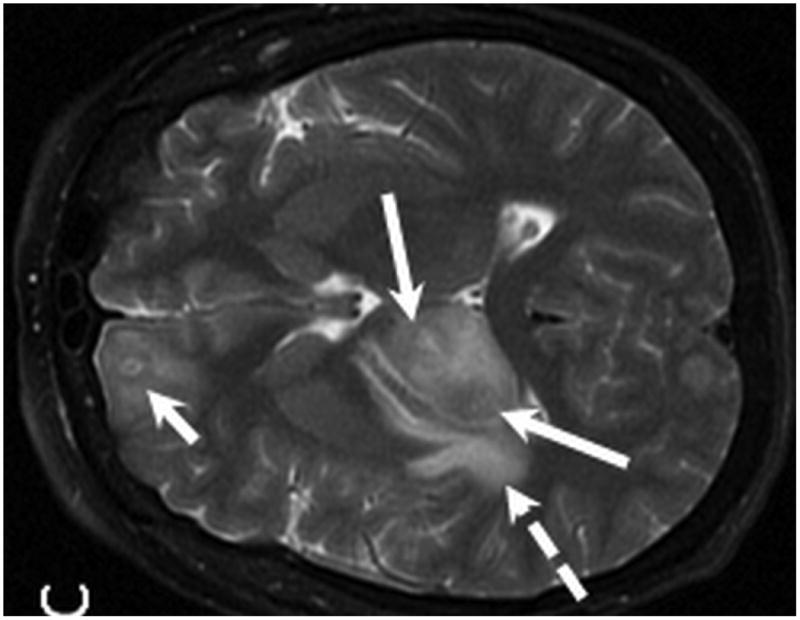
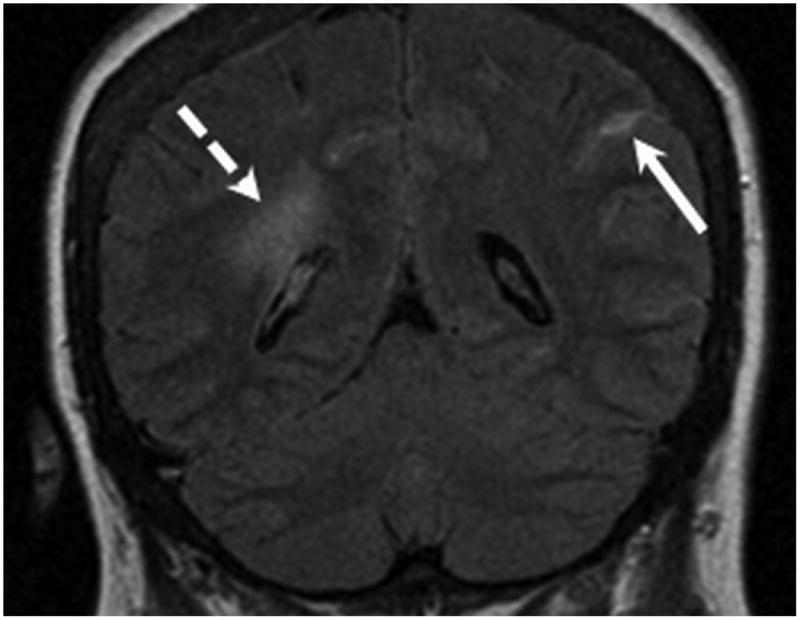
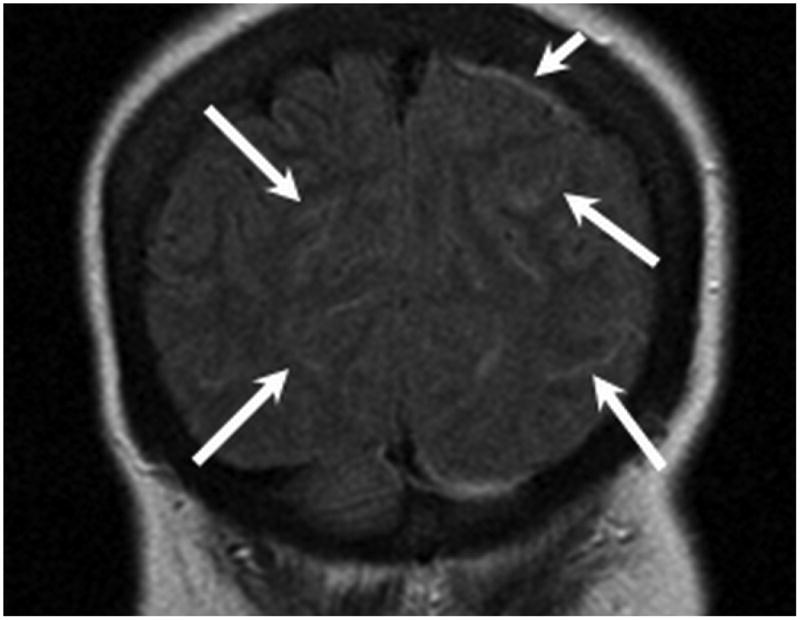
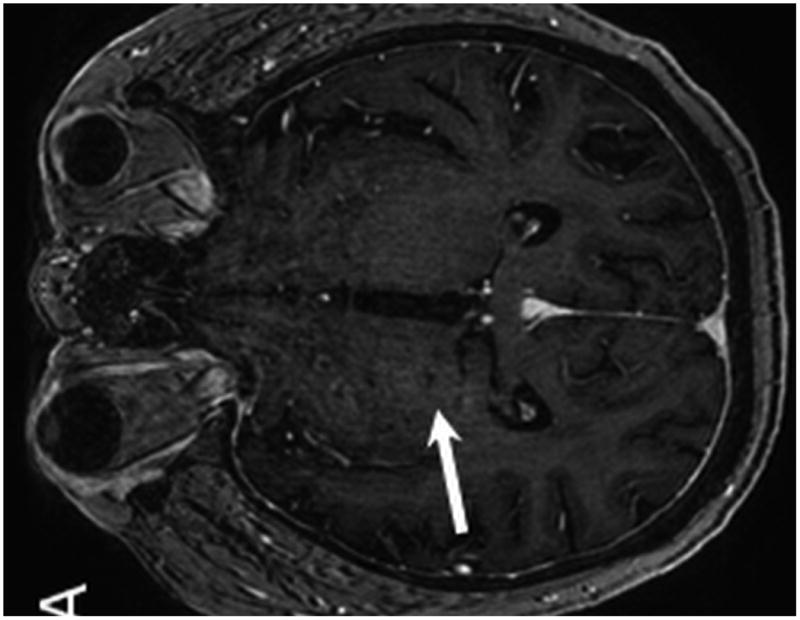
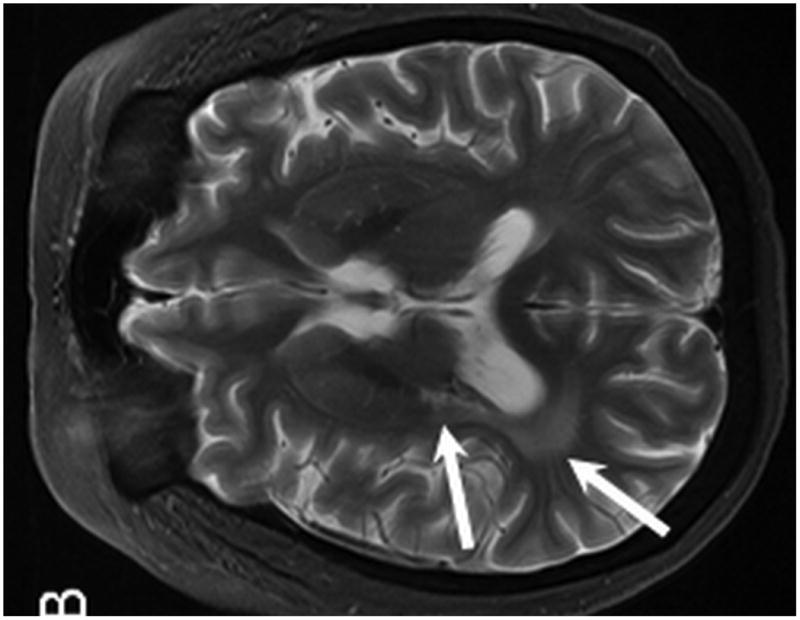
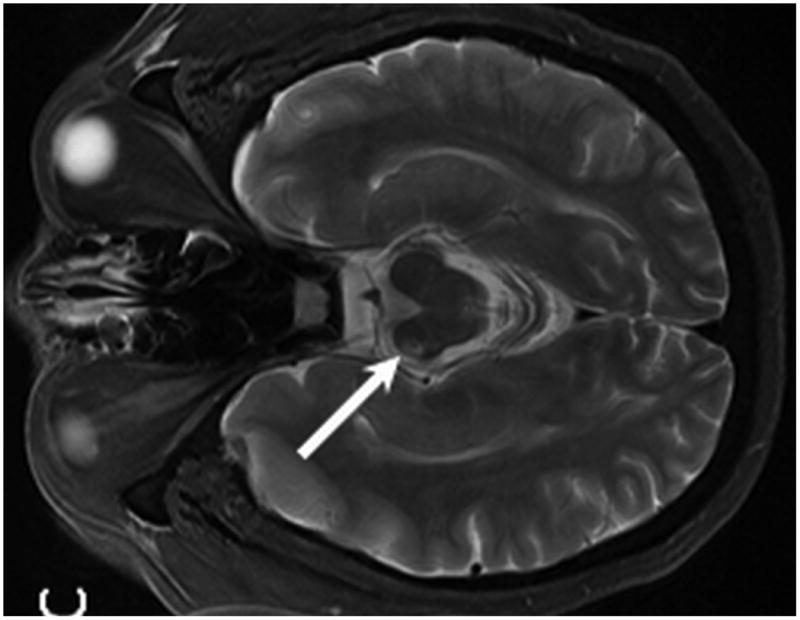
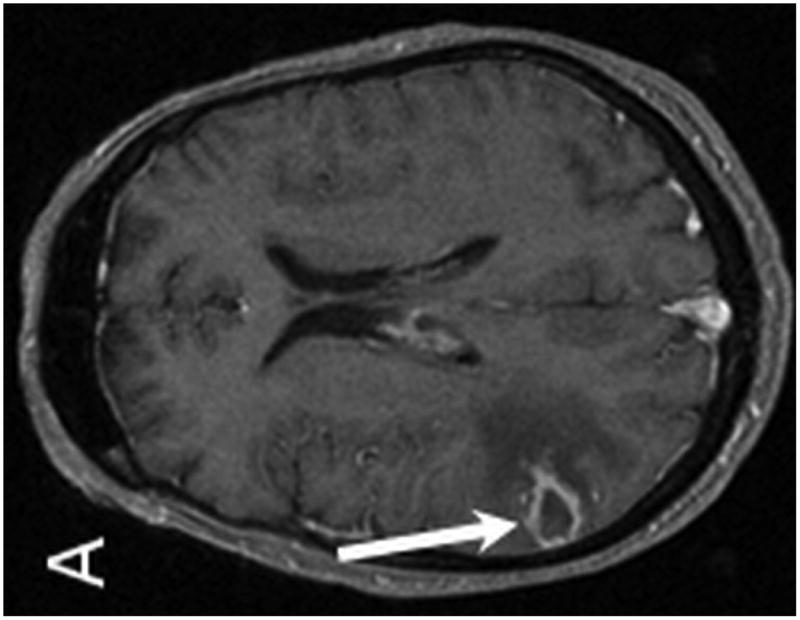
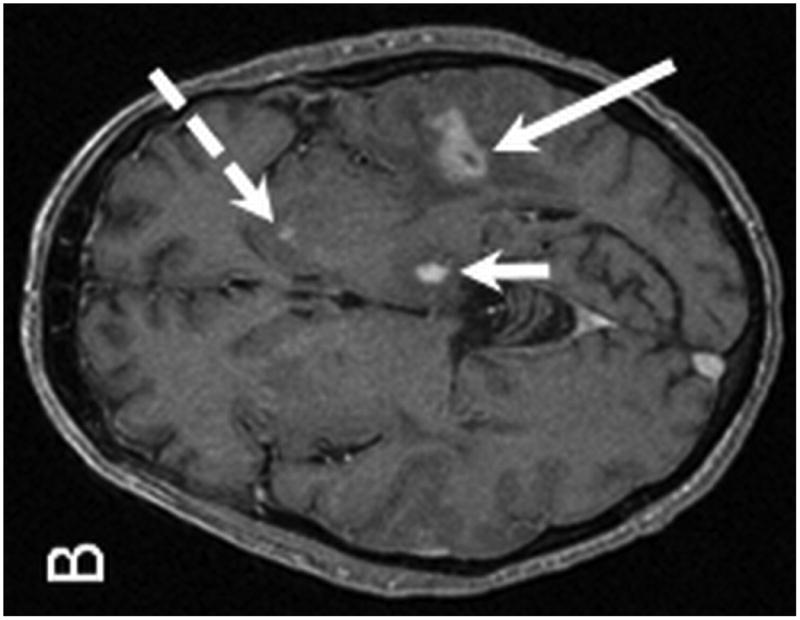
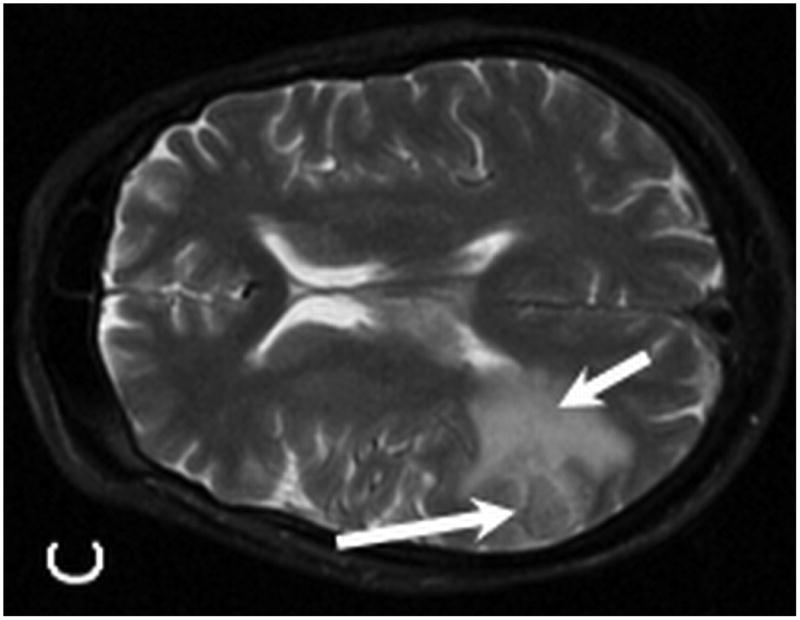
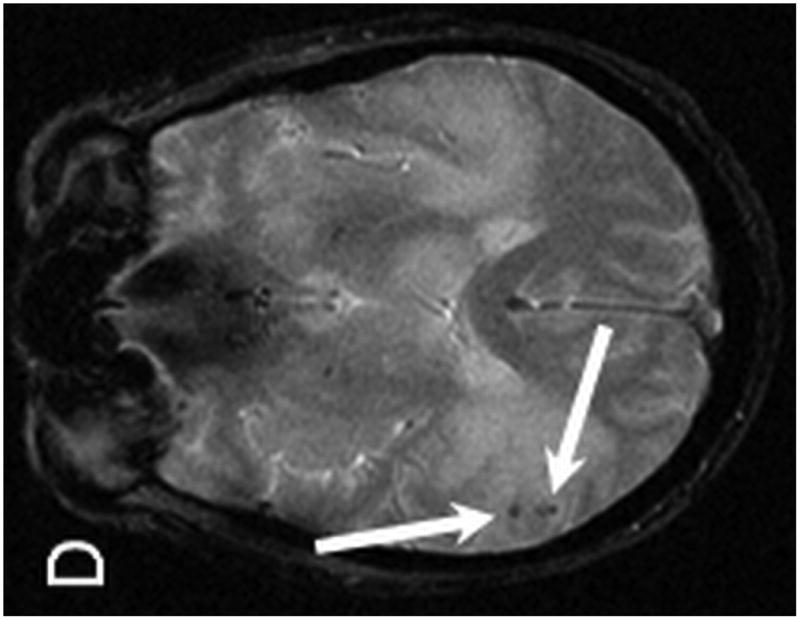
Results: All patients had kidney transplantation, and 3 had concurrent pancreas transplantation. Median age at diagnosis was 49 years, with a median of 4.5 years from SOT to diagnosis (range, 1.8-11.4 years). Presenting symptoms most often included focal neurological deficits (n = 6), although several patients had nonspecific symptoms of headache and altered mental status. Brain lesions were generally multiple (n = 7), supratentorial (n = 8), and lobar or periventricular in distribution with ring enhancement. Diagnosis was established by stereotactic (n = 4) and open surgical (n = 6) biopsy. Treatments most frequently administered included reduction of immunosuppression (n = 10), dexamethasone (n = 10), rituximab (n = 8), high-dose methotrexate (n = 3), and whole-brain radiotherapy (n = 6). Six patients remain alive without PCNS-PTLD relapse, including 4 patients who have sustained remissions beyond 2 years from diagnosis of PCNS-PTLD. Of 4 observed deaths, 1 was related to progressive PCNS-PTLD.
Conclusion: PCNS-PTLD must be considered in the differential diagnosis of any patient with prior SOT presenting with an intracranial lesion. Histological diagnosis with brain biopsy is imperative, given the risk for opportunistic infections that may have similar imaging findings and presentation. Prognosis is variable, although long-term survival has been reported.
Conflict of interest statement
Figures
References
-
- Penn I, Porat G. Central nervous system lymphomas in organ allograft recipients. Transplantation. 1995 Jan 27;59(2):240–244. - PubMed
-
- Castellano-Sanchez AA, Li S, Qian J, Lagoo A, Weir E, Brat DJ. Primary central nervous system posttransplant lymphoproliferative disorders. Am J Clin Pathol. 2004 Feb;121(2):246–253. - PubMed
-
- Gallardo D, Ferra C, Berlanga JJ, et al. Neurologic complications after allogeneic bone marrow transplantation. Bone Marrow Transplant. 1996 Dec;18(6):1135–1139. - PubMed
-
- Jamali FR, Otrock ZK, Soweid AM, et al. An overview of the pathogenesis and natural history of post-transplant T-cell lymphoma (corrected and republished article originally printed in Leukemia & Lymphoma, June 2007; 48(6): 1237 - 1241) Leuk Lymphoma. 2007 Sep;48(9):1780–1784. - PubMed
-
- Kim IY, Jung S, Jung TY, Kang SS, Choi C. Primary central nervous system lymphoma presenting as an acute massive intracerebral hemorrhage: case report with immunohistochemical study. Surg Neurol. 2008 Sep;70(3):308–311. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
