

Clinical outcomes in patients with stage I non-seminomatous germ cell cancer
- PMID: 23685909
- PMCID: PMC3739228
- DOI: 10.1038/aja.2013.16
Clinical outcomes in patients with stage I non-seminomatous germ cell cancer
Abstract
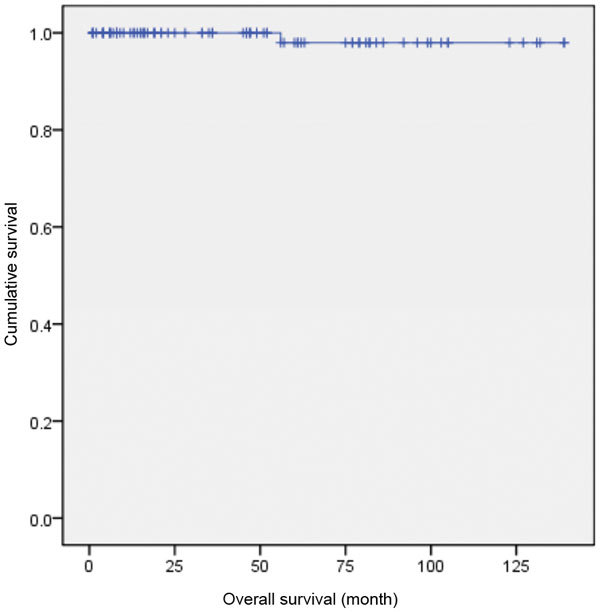
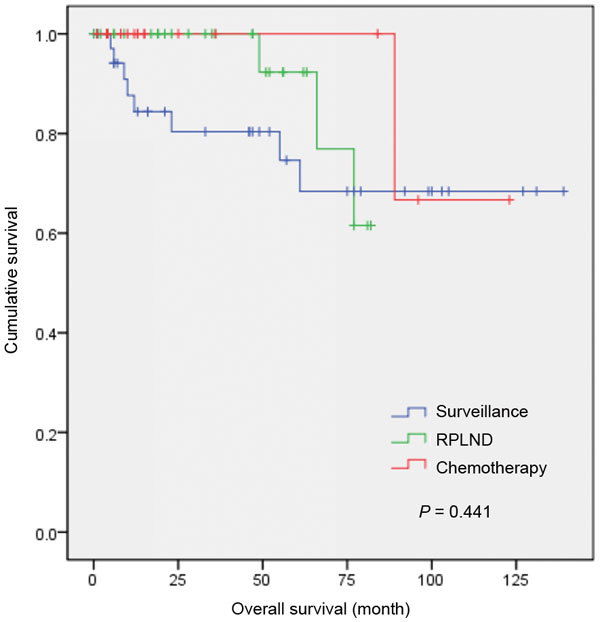
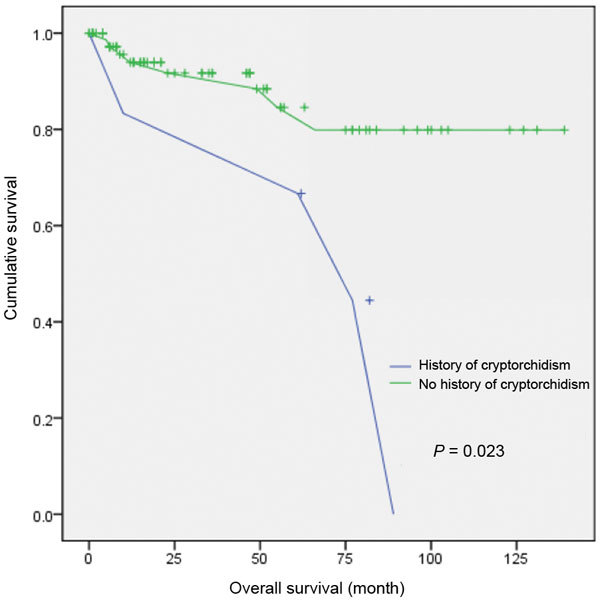
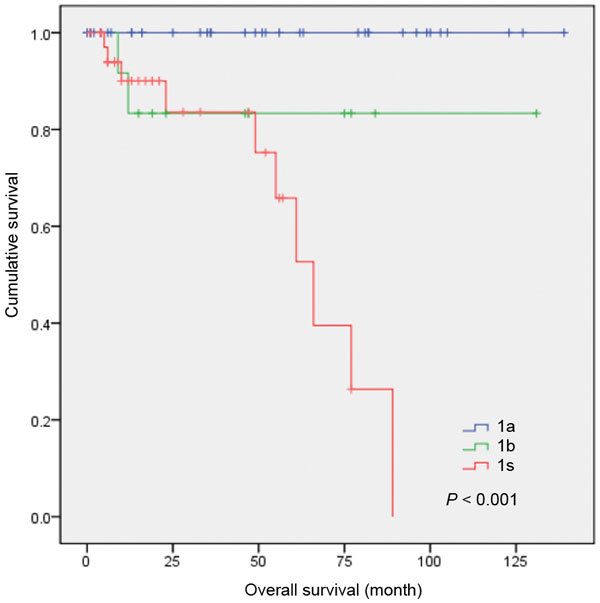
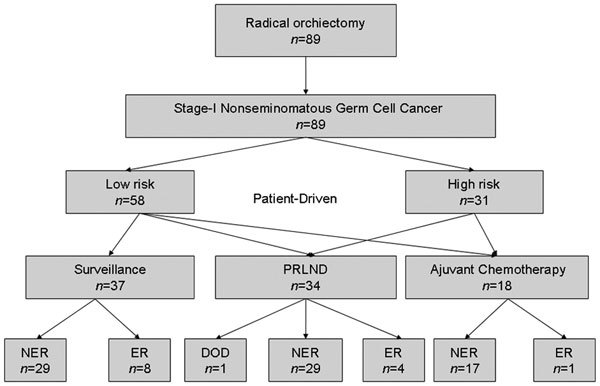
This study assesses the long-term outcomes in Han Chinese patients with clinical stage I non-seminomatous germ cell testicular cancer (CSI NSGCT) treated with surveillance, retroperitoneal lymph node dissection (RPLND) and adjuvant chemotherapy. We retrospectively evaluated 89 patients with a mean age of 26.5 years. After orchiectomy, 37 patients were treated with surveillance, 34 underwent RPLND and 18 were managed with chemotherapy. The overall survival rate, the recurrence-free survival rate and the risk factors were evaluated. The median follow-up length was 92 months (range: 6-149 months). Thirteen of the 89 patients (14.6%) had relapses, and one died by the evaluation date. The overall survival rate was 98.9%. The cumulative 4-year recurrence-free rates were 80.2%, 92.0% and 100% for the surveillance, RPLND and chemotherapy groups, respectively. The disease-free period tended to be briefer in patients with a history of cryptorchidism and those with stage Is. Therefore, surveillance, RPLND and adjuvant chemotherapy might be reliable strategies in compliant patients with CSI NSGCT. Surveillance should be recommended for patients with the lowest recurrence rate, especially those without lymphovascular invasion. This study might aid the establishment of a standard therapy for CSI NSGCT in China.
Figures
Similar articles
-
[Efficacy of modified retroperitoneal lymph node dissection for testicular nonseminomatous germ cell tumors].Ai Zheng. 2008 Dec;27(12):1302-6. Ai Zheng. 2008. PMID: 19079998 Chinese.
-
Randomized phase III trial comparing retroperitoneal lymph node dissection with one course of bleomycin and etoposide plus cisplatin chemotherapy in the adjuvant treatment of clinical stage I Nonseminomatous testicular germ cell tumors: AUO trial AH 01/94 by the German Testicular Cancer Study Group.J Clin Oncol. 2008 Jun 20;26(18):2966-72. doi: 10.1200/JCO.2007.12.0899. Epub 2008 May 5. J Clin Oncol. 2008. PMID: 18458040 Clinical Trial.
-
Comparative Effectiveness of Risk-adapted Surveillance vs Retroperitoneal Lymph Node Dissection in Clinical Stage I Nonseminomatous Germ Cell Testicular Cancer: A Retrospective Follow-up Study of 81 Patients.Asian Pac J Cancer Prev. 2015;16(8):3267-72. doi: 10.7314/apjcp.2015.16.8.3267. Asian Pac J Cancer Prev. 2015. PMID: 25921130
-
Management of patients with low-stage nonseminomatous germ cell testicular cancer.Curr Treat Options Oncol. 2005 Sep;6(5):367-77. doi: 10.1007/s11864-005-0040-z. Curr Treat Options Oncol. 2005. PMID: 16107240 Review.
-
Primary and Postchemotherapy Retroperitoneal Lymphadenectomy for Testicular Cancer.Oncol Res Treat. 2018;41(6):370-378. doi: 10.1159/000489508. Epub 2018 May 17. Oncol Res Treat. 2018. PMID: 29772568 Review.
Cited by
-
Current management and management controversies in early- and intermediate-stage of nonseminoma germ cell tumors.Transl Androl Urol. 2020 Jan;9(Suppl 1):S45-S55. doi: 10.21037/tau.2019.05.14. Transl Androl Urol. 2020. PMID: 32055485 Free PMC article. Review.
-
Trans- and extraperitoneal retroperitoneal lymph node dissection (RPLND) in the treatment for nonseminomatous germ cell testicular tumors (NSGCT): a single Chinese center's retrospective analysis.Int Urol Nephrol. 2014 Feb;46(2):363-9. doi: 10.1007/s11255-013-0547-3. Epub 2013 Sep 1. Int Urol Nephrol. 2014. PMID: 23996573
-
Systemic therapy for primary and extragonadal germ cell tumors: prognosis and nuances of treatment.Transl Androl Urol. 2020 Jan;9(Suppl 1):S56-S65. doi: 10.21037/tau.2019.09.11. Transl Androl Urol. 2020. PMID: 32055486 Free PMC article. Review.
-
Testicular germ cell tumours' clinical stage I: comparison of surveillance with adjuvant treatment strategies regarding recurrence rates and overall survival-a systematic review.World J Urol. 2022 Dec;40(12):2889-2900. doi: 10.1007/s00345-022-04145-6. Epub 2022 Sep 15. World J Urol. 2022. PMID: 36107211 Free PMC article.
References
-
- Huyghe E, Matsuda T, Thonneau P. Increasing incidence of testicular cancer worldwide: a review. J Urol. 2003;170:5–11. - PubMed
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. - PubMed
-
- Garner MJ, Turner MC, Ghadirian P, Krewski D. Epidemiology of testicular cancer: an overview. Int J Cancer. 2005;116:331–9. - PubMed
-
- National Comprehensive Network . NCCN Clinical Practice Guidelines in Oncology Testicular Cancer, version 1. Fort Washington, PA; NCCN; 2012;
-
- Brydoy M, Fossa SD, Klepp O, Bremnes RM, Wist EA, et al. Paternity following treatment for testicular cancer. J Natl Cancer Inst. 2005;97:1580–8. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
