

Outcomes in head and neck reconstruction by surgical site and donor site
- PMID: 23686870
- PMCID: PMC3695001
- DOI: 10.1002/lary.23775
Outcomes in head and neck reconstruction by surgical site and donor site
Abstract
Objectives/hypothesis: Define surgical outcomes of specific donor sites for free tissue transfer in head and neck reconstruction.
Study design: Retrospective cohort review at an academic tertiary care center.
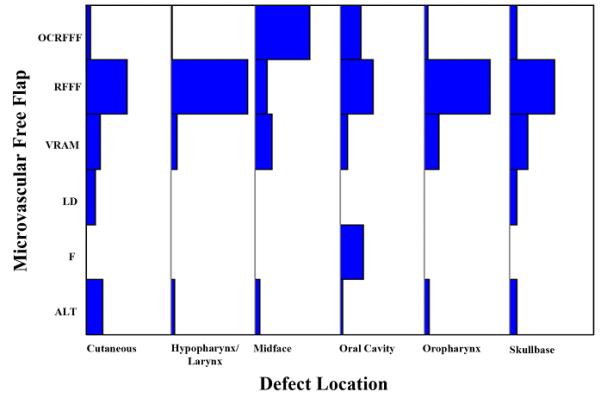
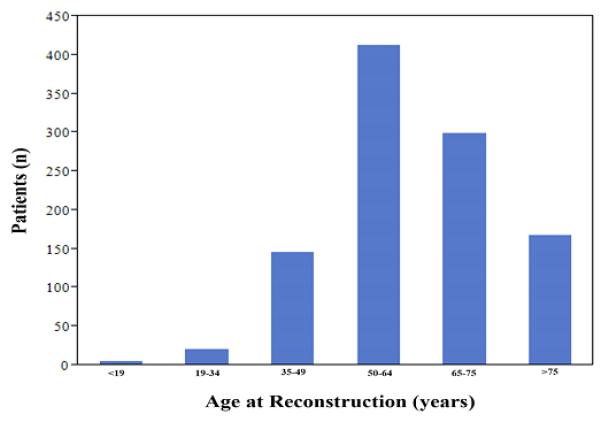
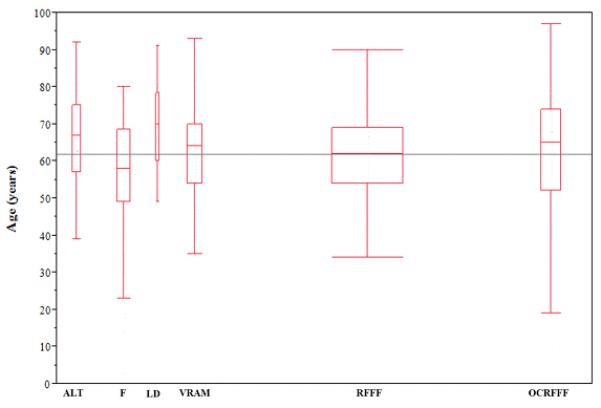
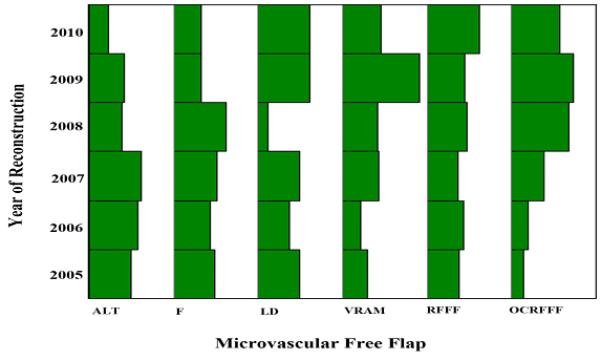
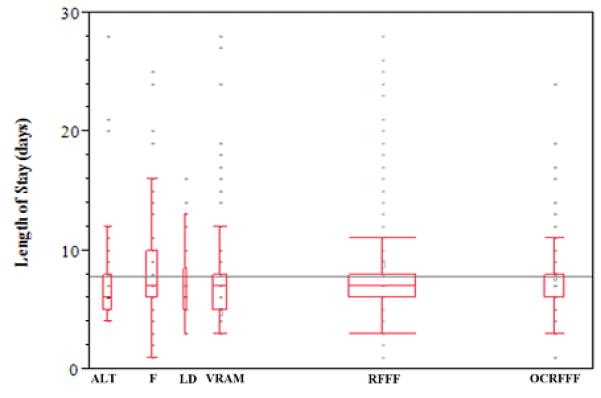
Methods: A review was made of free tissue transfer procedures performed at a university-based tertiary care facility from October 2004 to April 2011. A total of 1,051 patients underwent six types of free flaps: fasciocutaneous radial forearm (53%), osteocutaneous radial forearm (16%), rectus abdominis (11%), fibula (10%), anterior lateral thigh (7%), and latissimus dorsi (2%). Demographic data were collected, and outcomes measured were: length of hospital stay, flap viability, and major complications (infection, fistula, and hematoma).
Results: Of the 1,051 flaps performed, the most common operative site was oral cavity (40%, n = 414) followed by hypopharynx/larynx (22%, n = 234), cutaneous (20%, n = 206), oropharynx (9%, n = 98), midface (7%, n = 76), and skull base (2%, n = 23). The median hospital stay was 7.9 days (range, 1-76), and the overall failure rate was 2.8%. Cutaneous defects required the shortest length of hospitalization (5.8 days, P < .0001), a low free flap failure rate (1.5%, n = 3), and limited major complications (6%, n = 12). Conversely, oropharynx defects were associated with the longest hospitalization (8.9 days). Midface defects had a high incidence of complications (15%, n = 11, P = .10). Defects above the angle of the mandible had higher overall complications when compared to below. Similarly, reconstruction for primary or recurrent cancer had a total failure rate of 2.5%, whereas secondary reconstruction and radionecrosis had a failure rate of 4.0% (P = .29). Additionally, there was no statistical difference between outcomes based on donor site.
Conclusions: This review demonstrates that certain subsets of patients are at higher risk for complications after free tissue transfer. Patients undergoing free flap reconstruction for cutaneous defects have substantially shorter hospital stays and are at lower risk of flap complications, whereas reconstruction for radionecrosis and secondary reconstruction tend to have higher overall flap failure rates.
Copyright © 2013 The American Laryngological, Rhinological and Otological Society, Inc.
Figures
References
-
- Nakatsuka T, Harii K, Asato H, et al. Analytic review of 2372 free flap transfers for head and neck reconstruction following cancer resection. J Reconstr Microsurg. 2003;19:363–368. discussion 369. - PubMed
-
- Rinaldo A, Shaha AR, Wei WI, Silver CE, Ferlito A. Microvascular free flaps: a major advance in head and neck reconstruction. Acta Otolaryngol. 2002;122:779–784. - PubMed
-
- Seidenberg B, Hurwitt ES. Immediate reconstruction of the cervical esophagus by a revascularized isolated jejunal segment. Surg Forum. 1958;9:413–416. - PubMed
-
- Rosenthal E, Carroll W, Dobbs M, Scott Magnuson J, Wax M, Peters G. Simplifying head and neck microvascular reconstruction. Head Neck. 2004;26:930–936. - PubMed
-
- Disa JJ, Cordeiro PG. Mandible reconstruction with microvascular surgery. Semin Surg Oncol. 2000;19:226–234. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
