

Associations of visceral and abdominal subcutaneous adipose tissue with markers of cardiac and metabolic risk in obese adults
- PMID: 23687099
- PMCID: PMC3751977
- DOI: 10.1002/oby.20135
Associations of visceral and abdominal subcutaneous adipose tissue with markers of cardiac and metabolic risk in obese adults
Abstract
Objective: Visceral (VAT) and abdominal subcutaneous (SAT) adipose tissues contribute to obesity but may have different metabolic and atherosclerosis risk profiles. We sought to determine the associations of abdominal VAT and SAT mass with markers of cardiac and metabolic risk in a large, multiethnic, population-based cohort of obese adults.
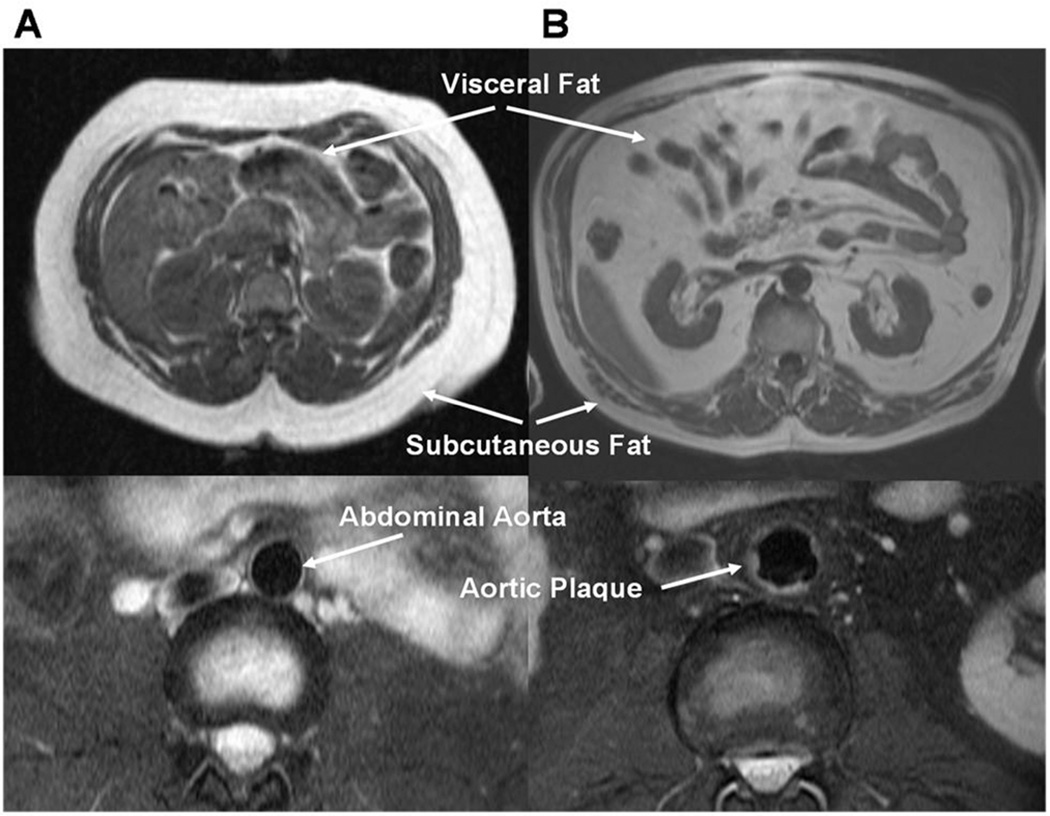
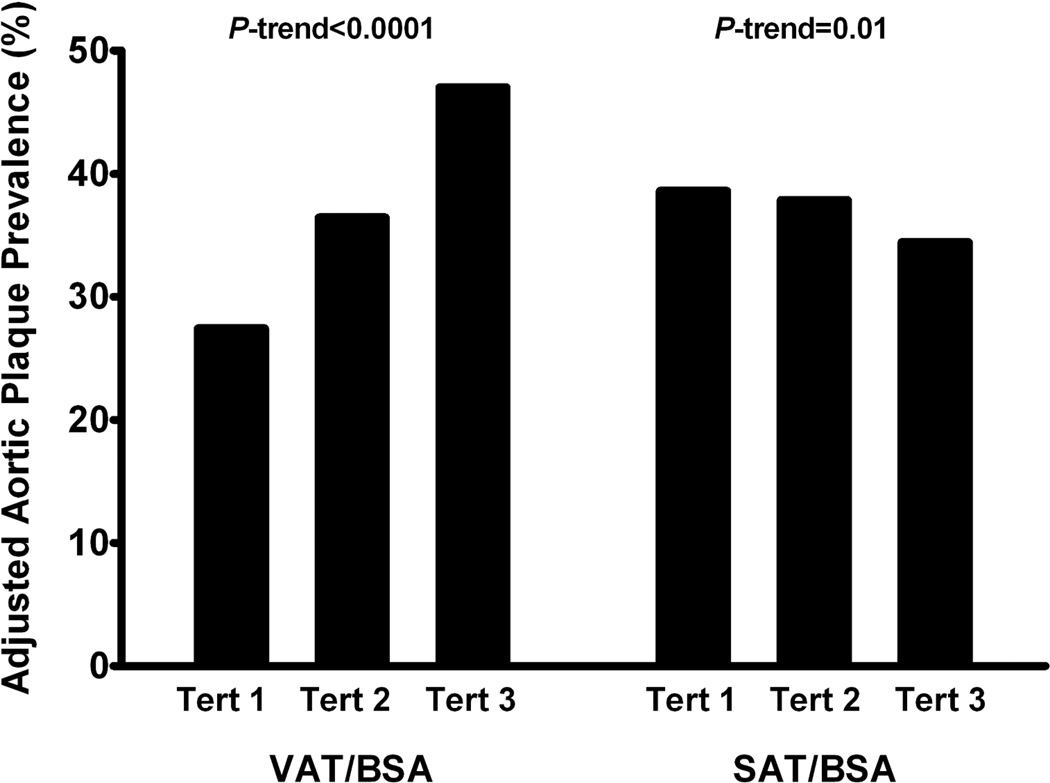
Design and methods: Among obese participants in the Dallas Heart Study, we examined the cross-sectional associations of abdominal VAT and SAT mass, assessed by magnetic resonance imaging (MRI) and indexed to body surface area (BSA), with circulating biomarkers of insulin resistance, dyslipidemia, and inflammation (n = 942); and with aortic plaque and liver fat by MRI and coronary calcium by computed tomography (n = 1200). Associations of VAT/BSA and SAT/BSA were examined after adjustment for age, sex, race, menopause, and body mass index.
Results: In multivariable models, VAT significantly associated with the homeostasis model assessment of insulin resistance (HOMA-IR), lower adiponectin, smaller LDL and HDL particle size, larger VLDL size, and increased LDL and VLDL particle number (p < 0.001 for each). VAT also associated with prevalent diabetes, metabolic syndrome, hepatic steatosis, and aortic plaque (p < 0.001 for each). VAT independently associated with C-reactive protein but not with any other inflammatory biomarkers tested. In contrast, SAT associated with leptin and inflammatory biomarkers, but not with dyslipidemia or atherosclerosis. Associations between SAT and HOMA-IR were significant in univariable analyses but attenuated after multivariable adjustment.
Conclusion: VAT associated with an adverse metabolic, dyslipidemic, and atherogenic obesity phenotype. In contrast, SAT demonstrated a more benign phenotype, characterized by modest associations with inflammatory biomarkers and leptin, but no independent association with dyslipidemia, insulin resistance, or atherosclerosis in obese individuals. These findings suggest that abdominal fat distribution defines distinct obesity sub-phenotypes with heterogeneous metabolic and atherosclerosis risk.
Copyright © 2012 The Obesity Society.
Figures
References
-
- Cornier MA, Despres JP, Davis N, et al. Assessing Adiposity: A Scientific Statement From the American Heart Association. Circulation. 2011;124:1996–2019. - PubMed
-
- Bays HE, Gonzalez-Campoy JM, Bray GA, et al. Pathogenic potential of adipose tissue and metabolic consequences of adipocyte hypertrophy and increased visceral adiposity. Expert Rev Cardiovasc Ther. 2008;6:343–368. - PubMed
-
- Tan CY, Vidal-Puig A. Adipose tissue expandability: the metabolic problems of obesity may arise from the inability to become more obese. Biochem Soc Trans. 2008;36:935–940. - PubMed
-
- Fox CS, Massaro JM, Hoffmann U, et al. Abdominal visceral and subcutaneous adipose tissue compartments: association with metabolic risk factors in the Framingham Heart Study. Circulation. 2007;116:39–48. - PubMed
-
- Oka R, Miura K, Sakurai M, et al. Impacts of visceral adipose tissue and subcutaneous adipose tissue on metabolic risk factors in middle-aged Japanese. Obesity (Silver Spring) 2010;18:153–160. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
