

Evidence-based detection of pulmonary arterial hypertension in systemic sclerosis: the DETECT study
- PMID: 23687283
- PMCID: PMC4078756
- DOI: 10.1136/annrheumdis-2013-203301
Evidence-based detection of pulmonary arterial hypertension in systemic sclerosis: the DETECT study
Abstract
Objective: Earlier detection of pulmonary arterial hypertension (PAH), a leading cause of death in systemic sclerosis (SSc), facilitates earlier treatment. The objective of this study was to develop the first evidence-based detection algorithm for PAH in SSc.
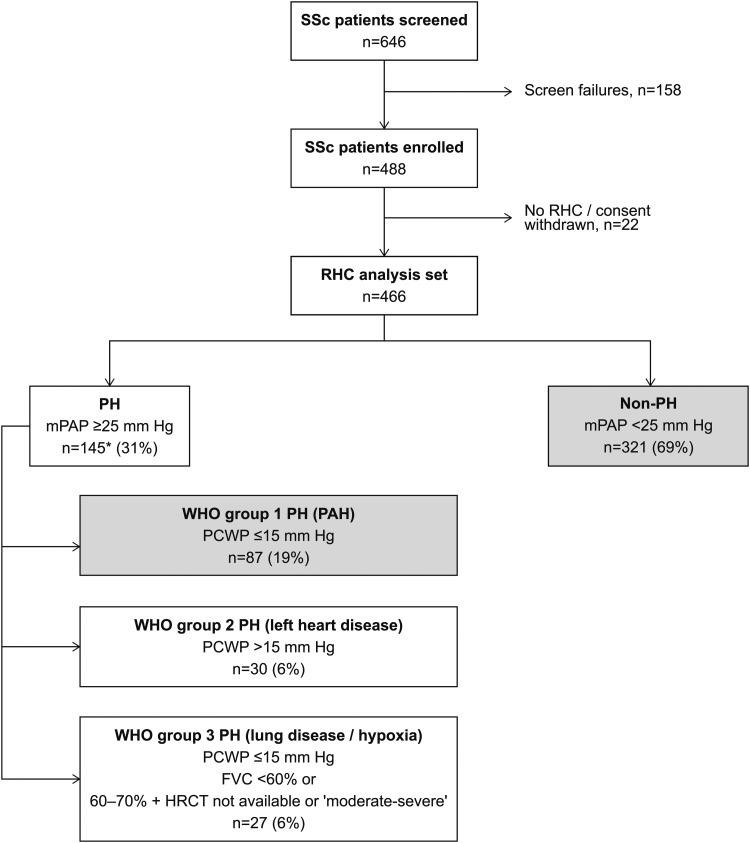
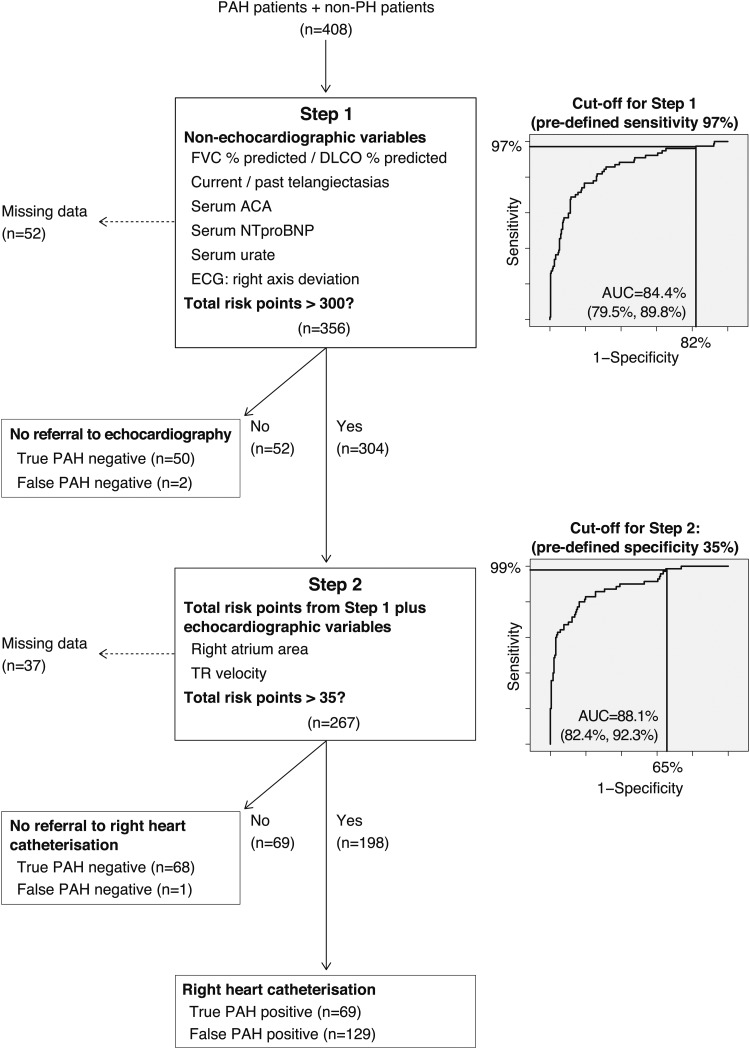
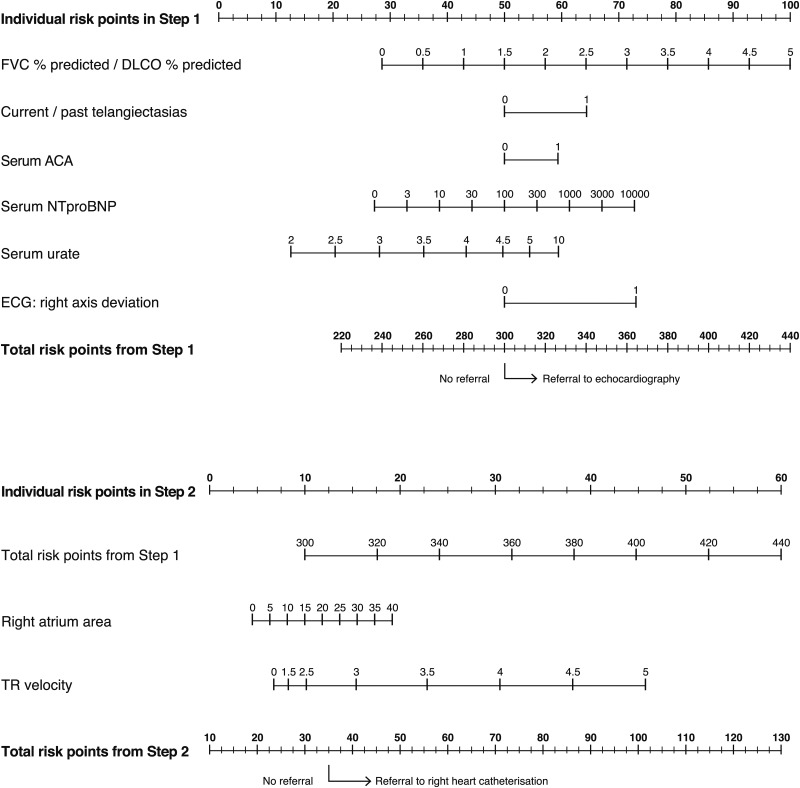
Methods: In this cross-sectional, international study conducted in 62 experienced centres from North America, Europe and Asia, adults with SSc at increased risk of PAH (SSc for >3 years and predicted pulmonary diffusing capacity for carbon monoxide <60%) underwent a broad panel of non-invasive assessments followed by diagnostic right heart catheterisation (RHC). Univariable and multivariable analyses selected the best discriminatory variables for identifying PAH. After assessment for clinical plausibility and feasibility, these were incorporated into a two-step, internally validated detection algorithm. Nomograms for clinical practice use were developed.
Results: Of 466 SSc patients at increased risk of PAH, 87 (19%) had RHC-confirmed PAH. PAH was mild (64% in WHO functional class I/II). Six simple assessments in Step 1 of the algorithm determined referral to echocardiography. In Step 2, the Step 1 prediction score and two echocardiographic variables determined referral to RHC. The DETECT algorithm recommended RHC in 62% of patients (referral rate) and missed 4% of PAH patients (false negatives). By comparison, applying European Society of Cardiology/European Respiratory Society guidelines to these patients, 29% of diagnoses were missed while requiring an RHC referral rate of 40%.
Conclusions: The novel, evidence-based DETECT algorithm for PAH detection in SSc is a sensitive, non-invasive tool which minimises missed diagnoses, identifies milder disease and addresses resource usage.
Keywords: Arterial Hypertension; Epidemiology; Systemic Sclerosis.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- Galiè N, Hoeper MM, Humbert M, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J 2009;30:2493–537 - PubMed
-
- McLaughlin VV, Archer SL, Badesch DB, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension: a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association: developed in collaboration with the American College of Chest Physicians, American Thoracic Society, Inc., and the Pulmonary Hypertension Association. Circulation 2009;119:2250–94 - PubMed
-
- Tyndall AJ, Bannet B, Vonk M, et al. Causes and risk factors for death in systemic sclerosis: a study from the EULAR Scleroderma Trial and Research (EUSTAR) database. Ann Rheum Dis 2010;69:1809–15 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
