

Inclusion of persons with mental illness in patient-centred medical homes: cross-sectional findings from Ontario, Canada
- PMID: 23687535
- PMCID: PMC3654503
Inclusion of persons with mental illness in patient-centred medical homes: cross-sectional findings from Ontario, Canada
Abstract
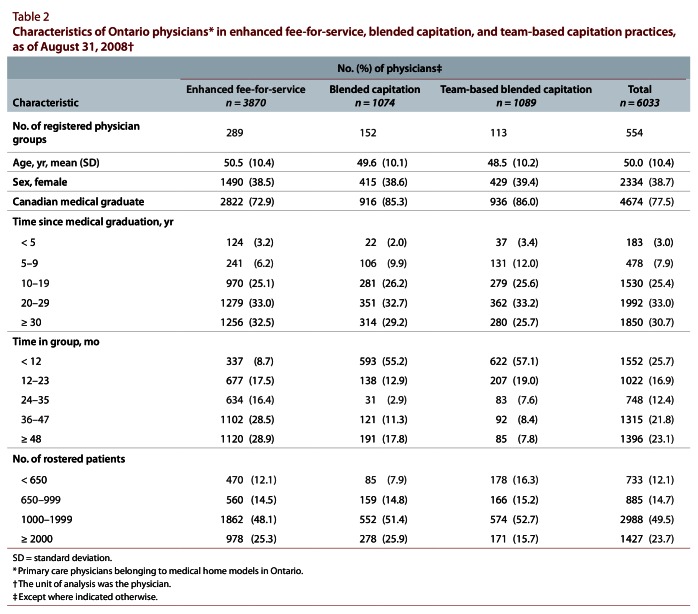
Background: In Ontario, Canada, the patient-centred medical home is a model of primary care delivery that includes 3 model types of interest for this study: enhanced fee-for-service, blended capitation, and team-based blended capitation. All 3 models involve rostering of patients and have similar practice requirements but differ in method of physician reimbursement, with the blended capitation models incorporating adjustments for age and sex, but not case mix, of rostered patients. We evaluated the extent to which persons with mental illness were included in physicians' total practices (as rostered and non-rostered patients) and were included on physicians' rosters across types of medical homes in Ontario.
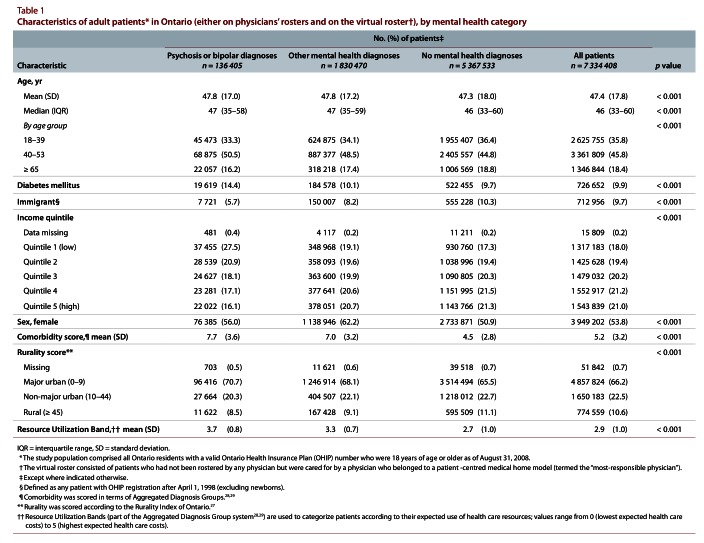
Methods: Using population-based administrative data, we considered 3 groups of patients: those with psychotic or bipolar diagnoses, those with other mental health diagnoses, and those with no mental health diagnoses. We modelled the prevalence of mental health diagnoses and the proportion of patients with such diagnoses who were rostered across the 3 medical home model types, controlling for demographic characteristics and case mix.
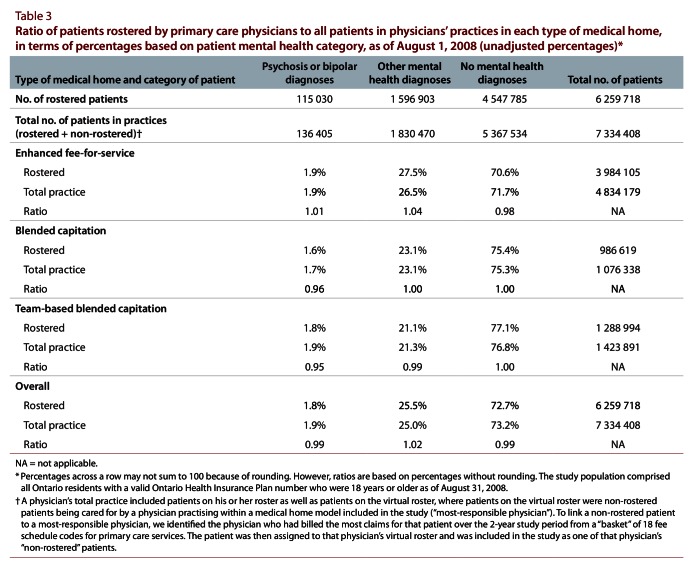
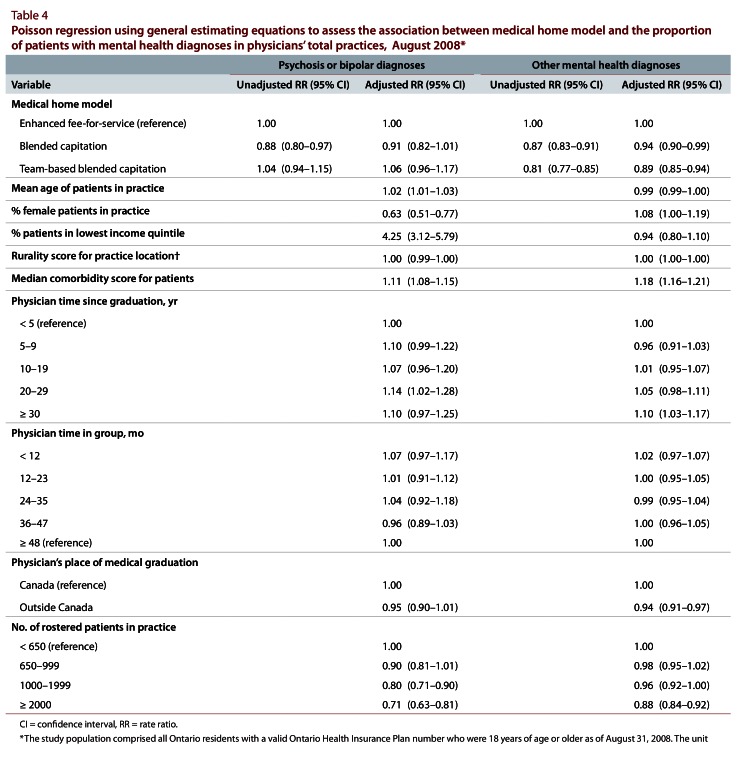
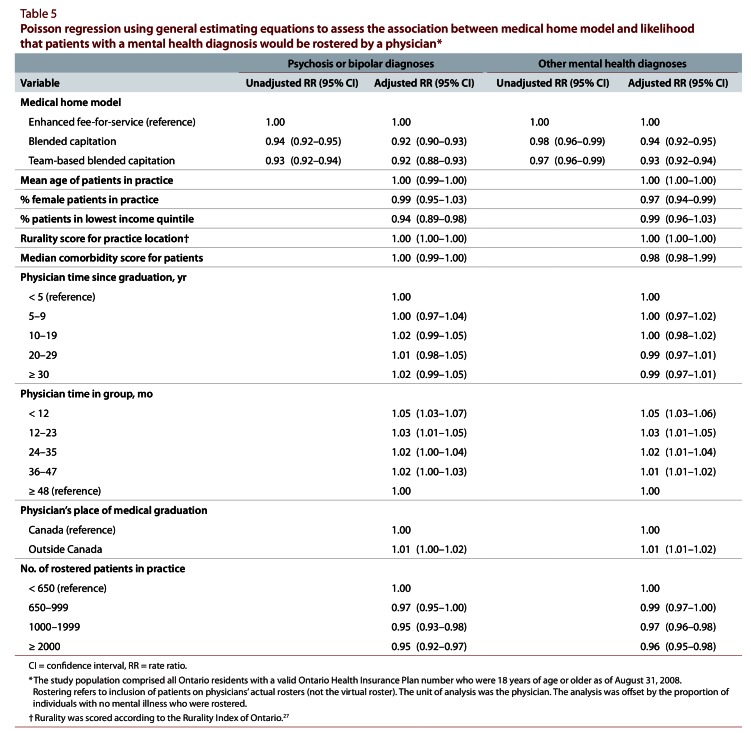
Results: Compared with enhanced fee-for-service practices, and relative to patients without mental illness, the proportions of patients with psychosis or bipolar disorders were not different in blended capitation and team-based blended capitation practices (rate ratio [RR] 0.91, 95% confidence interval [CI] 0.82-1.01; RR 1.06, 95% CI 0.96-1.17, respectively). However, there were fewer patients with other mental illnesses (RR 0.94, 95% CI 0.90-0.99; RR 0.89, 95% CI 0.85-0.94, respectively). Compared with expected proportions, practices based on both capitation models were significantly less likely than enhanced fee-for-service practices to roster patients with psychosis or bipolar disorders (for blended capitation, RR 0.92, 95% CI 0.90-0.93; for team-based capitation, RR 0.92, 95% CI 0.88-0.93) and also patients with other mental illnesses (for blended capitation, RR 0.94, 95% CI 0.92-0.95; for team-based capitation, RR 0.93, 95% CI 0.92-0.94).
Interpretation: Persons with mental illness were under-represented in the rosters of Ontario's capitation-based medical homes. These findings suggest a need to direct attention to the incentive structure for including patients with mental illness.
Conflict of interest statement
Competing interests: During the conduct of this study, Leah Steele received salary support in part through a Career Scientist Award from the Ontario Ministry of Health and Long-Term Care. No other competing interests declared.
Figures
Similar articles
-
Capitation and enhanced fee-for-service models for primary care reform: a population-based evaluation.CMAJ. 2009 May 26;180(11):E72-81. doi: 10.1503/cmaj.081316. CMAJ. 2009. PMID: 19468106 Free PMC article.
-
Longitudinal evaluation of physician payment reform and team-based care for chronic disease management and prevention.CMAJ. 2015 Nov 17;187(17):E494-E502. doi: 10.1503/cmaj.150579. Epub 2015 Sep 21. CMAJ. 2015. PMID: 26391722 Free PMC article.
-
Association of physician financial incentives with primary care enrolment of adults with serious mental illnesses in Ontario: a retrospective observational population-based study.CMAJ Open. 2023 Jan 10;11(1):E1-E12. doi: 10.9778/cmajo.20210190. Print 2023 Jan-Feb. CMAJ Open. 2023. PMID: 36627127 Free PMC article.
-
Mental Health Services Provision in Primary Care and Emergency Department Settings: Analysis of Blended Fee-for-Service and Blended Capitation Models in Ontario, Canada.Adm Policy Ment Health. 2021 Jul;48(4):654-667. doi: 10.1007/s10488-020-01099-y. Epub 2021 Jan 5. Adm Policy Ment Health. 2021. PMID: 33398538
-
Reimbursement Mechanisms and Challenges in Team-Based Behavioral Health Care: Issue Brief [Internet].Washington (DC): Office of the Assistant Secretary for Planning and Evaluation (ASPE); 2023 Oct 17. Washington (DC): Office of the Assistant Secretary for Planning and Evaluation (ASPE); 2023 Oct 17. PMID: 39250590 Free Books & Documents. Review.
Cited by
-
Can Collaborative Care Cure the Mediocrity of Usual Care for Common Mental Disorders?Can J Psychiatry. 2018 Jul;63(7):427-431. doi: 10.1177/0706743717748884. Epub 2018 Jan 9. Can J Psychiatry. 2018. PMID: 29316806 Free PMC article. No abstract available.
-
Primary care reform and funding equity for mental health disorders in Ontario: a retrospective observational population-based study.CMAJ Open. 2020 Jun 19;8(2):E455-E461. doi: 10.9778/cmajo.20190153. Print 2020 Apr-Jun. CMAJ Open. 2020. PMID: 32561592 Free PMC article.
-
Patients With Head and Neck Cancer and High Health Care Costs: A Population-Based Study.JAMA Otolaryngol Head Neck Surg. 2025 Jul 17:e251976. doi: 10.1001/jamaoto.2025.1976. Online ahead of print. JAMA Otolaryngol Head Neck Surg. 2025. PMID: 40674044
-
Barriers and facilitators to primary care for people with mental health and/or substance use issues: a qualitative study.BMC Fam Pract. 2015 Oct 13;16:135. doi: 10.1186/s12875-015-0353-3. BMC Fam Pract. 2015. PMID: 26463083 Free PMC article.
-
Patient characteristics associated with enrolment under voluntary programs implemented within fee-for-service systems in British Columbia and Quebec: a cross-sectional study.CMAJ Open. 2022 Feb 1;10(1):E64-E73. doi: 10.9778/cmajo.20210043. Print 2022 Jan-Mar. CMAJ Open. 2022. PMID: 35105683 Free PMC article.
References
-
- Rosenthal Thomas C. The medical home: growing evidence to support a new approach to primary care. J Am Board Fam Med. 2008;21(5):427–440. doi: 10.3122/jabfm.2008.05.070287. http://www.scholaruniverse.com/ncbi-linkout?id=18772297. - DOI - PubMed
-
- Wang Philip S, Lane Michael, Olfson Mark, Pincus Harold A, Wells Kenneth B, Kessler Ronald C. Twelve-month use of mental health services in the United States: results from the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):629–640. doi: 10.1001/archpsyc.62.6.629. http://www.scholaruniverse.com/ncbi-linkout?id=15939840. - DOI - PubMed
-
- Hinshaw S P, Cicchetti D. Stigma and mental disorder: conceptions of illness, public attitudes, personal disclosure, and social policy. Dev Psychopathol. 2000;12(4):555–598. http://www.scholaruniverse.com/ncbi-linkout?id=11202034. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources