

Evidence of Endothelial Activation in Asymptomatic Plasmodium falciparum Parasitemia and Effect of Blood Group on Levels of von Willebrand Factor in Malaria
- PMID: 23687570
- PMCID: PMC3656549
- DOI: 10.1093/jpids/pis010
Evidence of Endothelial Activation in Asymptomatic Plasmodium falciparum Parasitemia and Effect of Blood Group on Levels of von Willebrand Factor in Malaria
Abstract
Background: Endothelial activation may contribute to development of severe disease from Plasmodium falciparum infection, but optimal markers of endothelial activation in severe malaria, the extent of endothelial activation in asymptomatic infection, and the effect of blood group O on endothelial activation have not been defined.
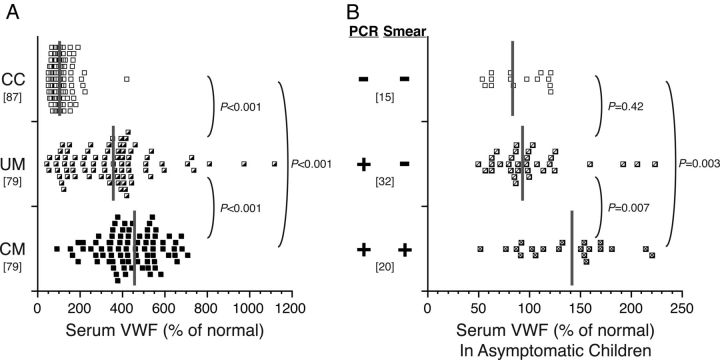
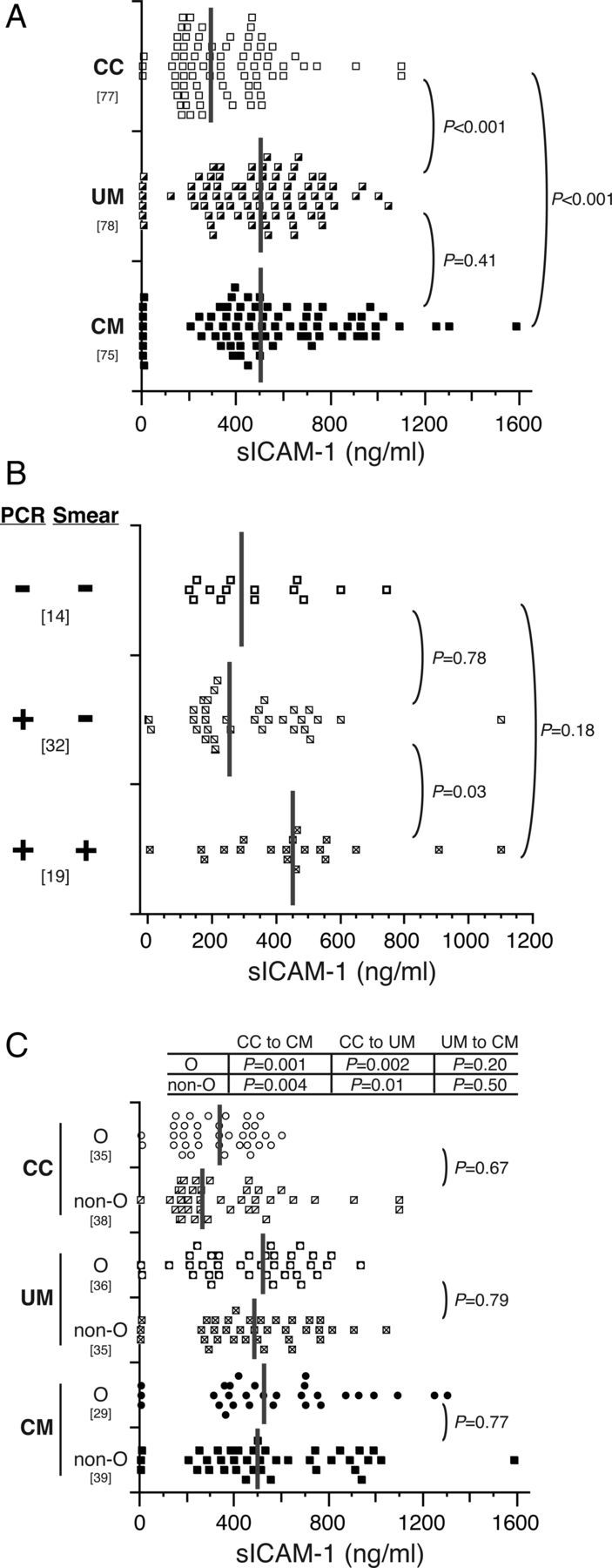
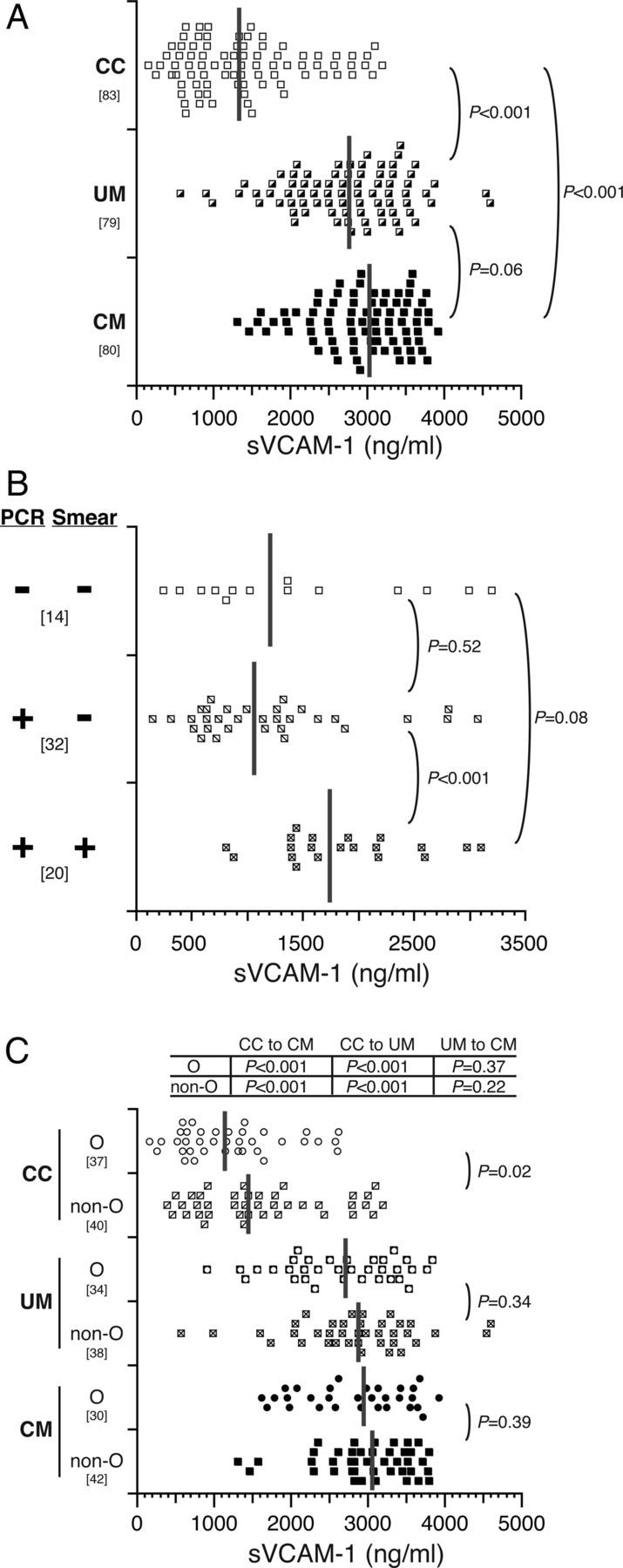
Methods: Serum levels of 3 markers of endothelial activation-von Willebrand factor (VWF), soluble intercellular adhesion molecule-1 (sICAM-1), and soluble vascular cell adhesion molecule-1 (sVCAM-1)-were assessed in Ugandan children with cerebral malaria (CM) (n = 86), children with uncomplicated malaria (UM) (n = 81), and community children (CC) (n = 90).
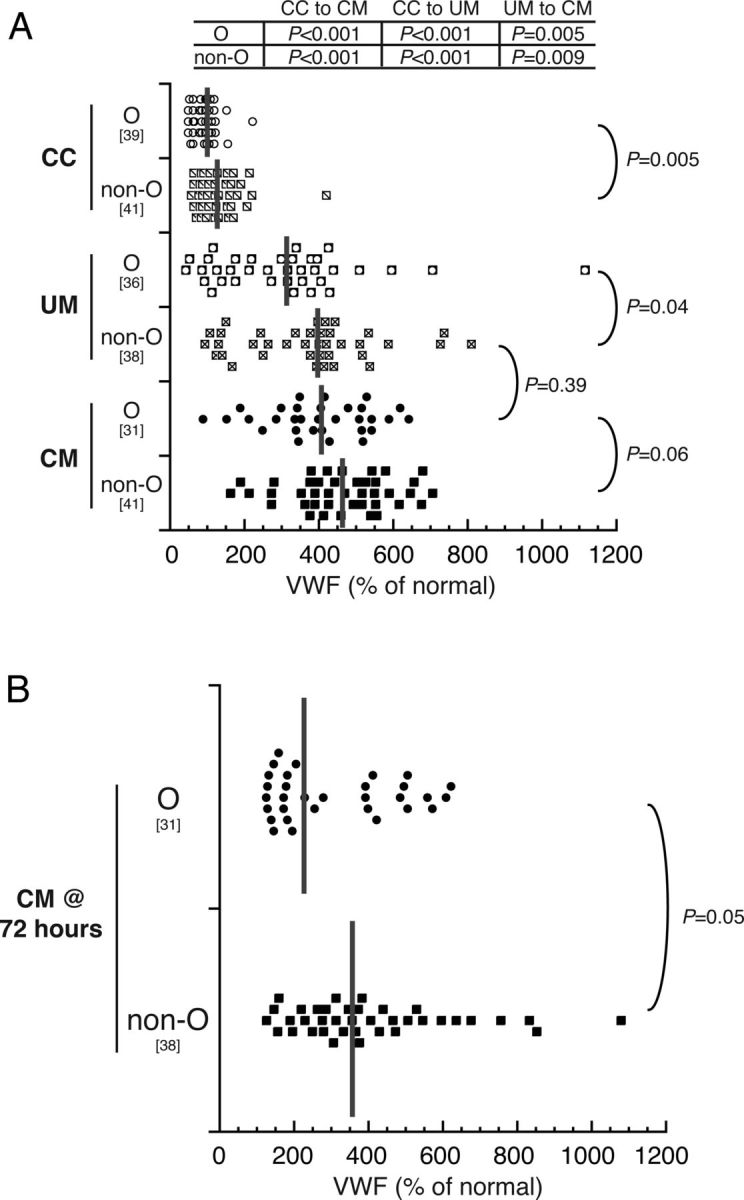
Results: Serum VWF, sICAM-1, and sVCAM-1 levels were all elevated in asymptomatic community children with microscopy-confirmed parasitemia when compared with children without parasitemia by microscopy or polymerase chain reaction (all, P ≤ .05). Levels of VWF, sICAM-1, and sVCAM-1 were higher in children with UM than in CC (all, P < 0.001), but only VWF levels effectively distinguished CM from UM (P < 0.001), a finding confirmed by receiver operating characteristic analyses (area under the curve = 0.67; 95% confidence interval, .58-.75). Von Willebrand factor levels were lower in children with blood group O versus non-O blood groups across the disease spectrum, but VWF levels remained higher in CM versus UM, even after controlling for blood group.
Conclusions: Endothelial activation, as assessed by serum levels of VWF, sICAM-1, and sVCAM-1, occurs even in subclinical P. falciparum parasitemia. Von Willebrand factor levels increase with greater malaria disease severity. Blood group O is associated with lower VWF levels, but presence of blood group O alone does not explain the higher VWF levels seen in children with CM.
Published by Oxford University Press on behalf of the Pediatric Infectious Diseases Society 2012.
Figures
Similar articles
-
Prognostic value of serum von Willebrand factor, but not soluble ICAM and VCAM, for mortality and cardiovascular events is independent of residual renal function in peritoneal dialysis patients.Perit Dial Int. 2014 Nov-Dec;34(7):706-13. doi: 10.3747/pdi.2012.00004. Epub 2014 Mar 1. Perit Dial Int. 2014. PMID: 24584618 Free PMC article.
-
Combined measurement of soluble and cellular ICAM-1 among children with Plasmodium falciparum malaria in Uganda.Malar J. 2010 Aug 16;9:233. doi: 10.1186/1475-2875-9-233. Malar J. 2010. PMID: 20712868 Free PMC article.
-
Effects of severe, uncontrolled hypertension on endothelial activation: soluble vascular cell adhesion molecule-1, soluble intercellular adhesion molecule-1 and von Willebrand factor.J Hypertens. 2002 May;20(5):871-7. doi: 10.1097/00004872-200205000-00021. J Hypertens. 2002. PMID: 12011647
-
Characterization of recessive severe type 1 and 3 von Willebrand Disease (VWD), asymptomatic heterozygous carriers versus bloodgroup O-related von Willebrand factor deficiency, and dominant type 1 VWD.Clin Appl Thromb Hemost. 2006 Jul;12(3):277-95. doi: 10.1177/1076029606291401. Clin Appl Thromb Hemost. 2006. PMID: 16959681 Review.
-
Coagulopathy in malaria.Thromb Res. 2014 Jan;133(1):5-9. doi: 10.1016/j.thromres.2013.09.030. Epub 2013 Sep 26. Thromb Res. 2014. PMID: 24099998 Review.
Cited by
-
Measuring soluble ICAM-1 in African populations.PLoS One. 2014 Oct 7;9(10):e108956. doi: 10.1371/journal.pone.0108956. eCollection 2014. PLoS One. 2014. PMID: 25289635 Free PMC article.
-
The spectrum of clinical biomarkers in severe malaria and new avenues for exploration.Virulence. 2022 Dec;13(1):634-653. doi: 10.1080/21505594.2022.2056966. Virulence. 2022. PMID: 36036460 Free PMC article. Review.
-
Experimental Models to Study the Pathogenesis of Malaria-Associated Acute Respiratory Distress Syndrome.Front Cell Infect Microbiol. 2022 May 23;12:899581. doi: 10.3389/fcimb.2022.899581. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 35677654 Free PMC article. Review.
-
Escaping the enemy's bullets: an update on how malaria parasites evade host immune response.Parasitol Res. 2023 Aug;122(8):1715-1731. doi: 10.1007/s00436-023-07868-6. Epub 2023 May 23. Parasitol Res. 2023. PMID: 37219610 Free PMC article. Review.
-
Von Willebrand Factor Facilitates Intravascular Dissemination of Microsporidia Encephalitozoon hellem.Front Cell Infect Microbiol. 2021 May 21;11:694957. doi: 10.3389/fcimb.2021.694957. eCollection 2021. Front Cell Infect Microbiol. 2021. PMID: 34095003 Free PMC article.
References
-
- Breman JG, Alilio MS, Mills A. Conquering the intolerable burden of malaria: what's new, what's needed: a summary. Am J Trop Med Hyg. 2004;71:1–15. - PubMed
-
- van der Heyde HC, Nolan J, Combes V, Gramaglia I, Grau GE. A unified hypothesis for the genesis of cerebral malaria: sequestration, inflammation and hemostasis leading to microcirculatory dysfunction. Trends Parasitol. 2006;22:503–8. - PubMed
-
- Haldar K, Murphy SC, Milner DA, Taylor TE. Malaria: mechanisms of erythrocytic infection and pathological correlates of severe disease. Annu Rev Pathol. 2007;2:217–49. - PubMed
-
- Clark IA, Rockett KA. The cytokine theory of human cerebral malaria. Parasitol Today. 1994;10:410–2. - PubMed
-
- Hollestelle MJ, Donkor C, Mantey EA, et al. von Willebrand factor propeptide in malaria: evidence of acute endothelial cell activation. Br J Haematol. 2006;133:562–9. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
