

Development of new measurement system of thoracic excursion with biofeedback: reliability and validity
- PMID: 23687911
- PMCID: PMC3669041
- DOI: 10.1186/1743-0003-10-45
Development of new measurement system of thoracic excursion with biofeedback: reliability and validity
Abstract
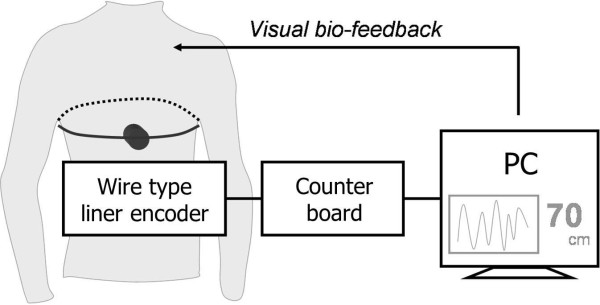
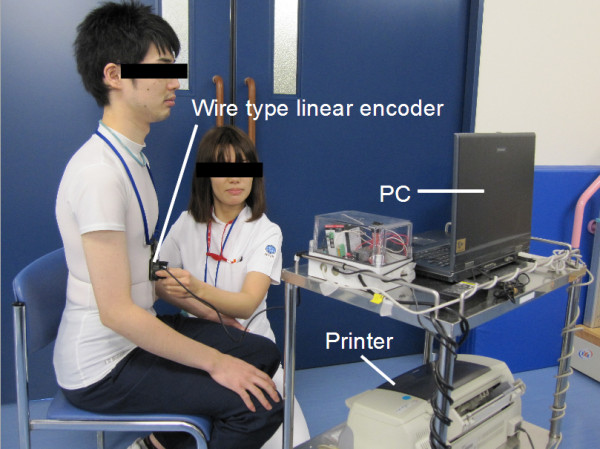
Background: Respiratory rehabilitation reduces breathlessness from patient with respiratory dysfunction. Chest expansion score, which represents the circumference magnitude of the thoracic cage, is used for a target when treating patients with respiratory disease. However, it is often difficult for patients to understand the changes in the respiratory status and be motivated for therapy continuously. We developed a new measurement system with biofeedback named BREATH which shows chest expansion scores in real time. The purpose of this study was to determine the reliability and validity of the novel system in advance of clinical application.
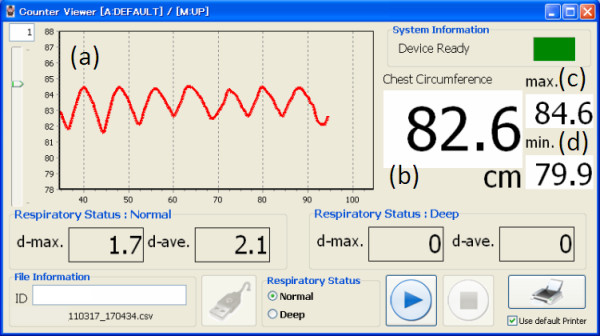
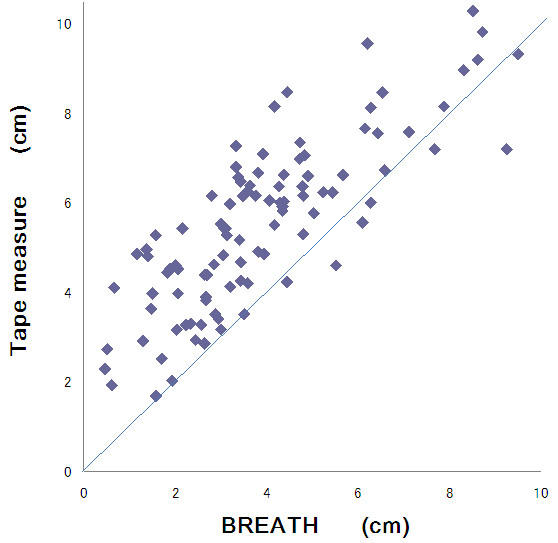
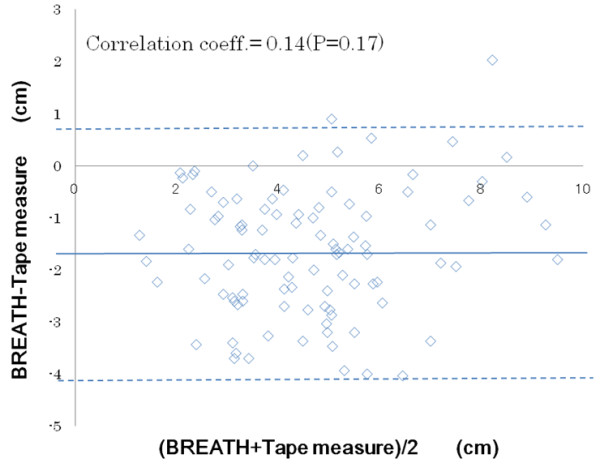
Methods: Three evaluators measured chest expansion in 33 healthy individuals using tape measure, which is used for the measurement traditionally, and BREATH. The wire for BREATH system was threaded over the thoracic continuously and the data was recorded automatically; whereas the tape was winded and measured each maximal expiration and inspiration timing by evaluator. All participants were performed both measurement simultaneously for three times during deep breath. In this study, we studied chest expansion score without using biofeedback data of BREATH to check the validity of the result. To confirm intra- and inter-evaluator reliability, we computed intra-class correlations (ICCs). We used Pearson's correlation coefficient to evaluate the validity of measurement result by BREATH with reference to the tape measure results.
Results: The average (standard deviation) chest expansion scores for all, men and women by the tape measure were 5.53 (1.88), 6.40 (1.69) and 5.22 (1.39) cm, respectively, and those by BREATH were 3.89 (2.04), 4.36 (1.83) and 2.89 (1.66) cm, respectively. ICC within and among the three evaluators for BREATH and the tape measure were 0.90-0.94 and 0.85-0.94 and 0.85 and 0.82, respectively. The correlation coefficient between the two methods was 0.76-0.87.
Conclusion: The novel measurement system, BREATH, has high intra- and inter-evaluator reliabilities and validity; therefore it can lead us more effective respiratory exercise. Using its biofeedback data, this system may help patients with respiratory disease to do exercises more efficiently and clinicians to assess the respiratory exercise more accurately.
Figures
Similar articles
-
Thoracic ROM measurement system with visual bio-feedback: system design and biofeedback evaluation.Annu Int Conf IEEE Eng Med Biol Soc. 2011;2011:1272-4. doi: 10.1109/IEMBS.2011.6090299. Annu Int Conf IEEE Eng Med Biol Soc. 2011. PMID: 22254548
-
Development and Pilot Test of a Virtual Reality Respiratory Biofeedback Approach.Appl Psychophysiol Biofeedback. 2020 Sep;45(3):153-163. doi: 10.1007/s10484-020-09468-x. Epub 2020 May 2. Appl Psychophysiol Biofeedback. 2020. PMID: 32361963 Free PMC article. Clinical Trial.
-
Respiratory feedback for treating panic disorder.J Clin Psychol. 2004 Feb;60(2):197-207. doi: 10.1002/jclp.10245. J Clin Psychol. 2004. PMID: 14724927
-
Development of a modular stress management platform (Performance Edge VR) and a pilot efficacy trial of a bio-feedback enhanced training module for controlled breathing.PLoS One. 2021 Feb 2;16(2):e0245068. doi: 10.1371/journal.pone.0245068. eCollection 2021. PLoS One. 2021. PMID: 33529187 Free PMC article.
-
RESPeRATE: the role of paced breathing in hypertension treatment.J Am Soc Hypertens. 2015 Jan;9(1):38-47. doi: 10.1016/j.jash.2014.10.002. Epub 2014 Oct 16. J Am Soc Hypertens. 2015. PMID: 25539897 Review.
Cited by
-
Effects of increased functional residual capacity on finger-floor distance in healthy young adults.J Phys Ther Sci. 2019 Jan;31(1):29-32. doi: 10.1589/jpts.31.29. Epub 2019 Jan 10. J Phys Ther Sci. 2019. PMID: 30774201 Free PMC article.
-
Thoracic Excursion Is a Biomarker for Evaluating Respiratory Function in Amyotrophic Lateral Sclerosis.Front Neurol. 2022 Mar 23;13:853469. doi: 10.3389/fneur.2022.853469. eCollection 2022. Front Neurol. 2022. PMID: 35401409 Free PMC article.
-
Serratus anterior fascia plane block for pain control in patients with multiple rib fractures.J Phys Ther Sci. 2023 Sep;35(9):673-677. doi: 10.1589/jpts.35.673. Epub 2023 Sep 2. J Phys Ther Sci. 2023. PMID: 37670765 Free PMC article.
-
Depth-Sensing-Based Algorithm for Chest Morphology Assessment in Children with Cerebral Palsy.Sensors (Basel). 2024 Aug 28;24(17):5575. doi: 10.3390/s24175575. Sensors (Basel). 2024. PMID: 39275488 Free PMC article.
-
The Breathing IQ: an anthropometric index of diaphragmatic breathing efficiency.Front Physiol. 2025 Apr 2;15:1394109. doi: 10.3389/fphys.2024.1394109. eCollection 2024. Front Physiol. 2025. PMID: 40242838 Free PMC article.
References
-
- Izumizaki M, Kakizaki F, Tanaka K, Homma I. Immediate effects of thixotropy conditioning of inspiratory muscles on chest wall volume in chronic obstructive pulmonary disease. Respir Care. 2006;51:750–757. - PubMed
-
- The Japan Society for Respiratory Care and Rehabilitation, The Japanese Respiratory Society, The Japanese Association of Rehabilitation Medicine, and The Japanese Physical Therapy Association: Current condition of respiratory rehabilitation. Guidelines for pulmonary rehabilitation: manual for exercise and training. Tokyo, JAPAN; 2003. pp. 17–28. in Japanese.
-
- Bockenhauer SE, Chen H, Julliard KN, Weedon J. Measuring thoracic excursion: reliability of the cloth tape measure technique. J Am Osteopath Assoc. 2007;107:191–196. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
