

A randomized trial of nighttime physician staffing in an intensive care unit
- PMID: 23688301
- PMCID: PMC3732473
- DOI: 10.1056/NEJMoa1302854
A randomized trial of nighttime physician staffing in an intensive care unit
Abstract
Background: Increasing numbers of intensive care units (ICUs) are adopting the practice of nighttime intensivist staffing despite the lack of experimental evidence of its effectiveness.
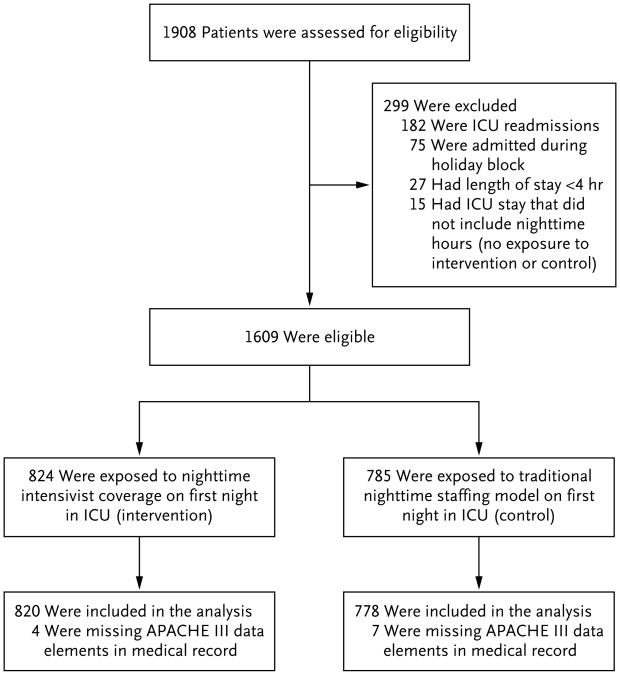
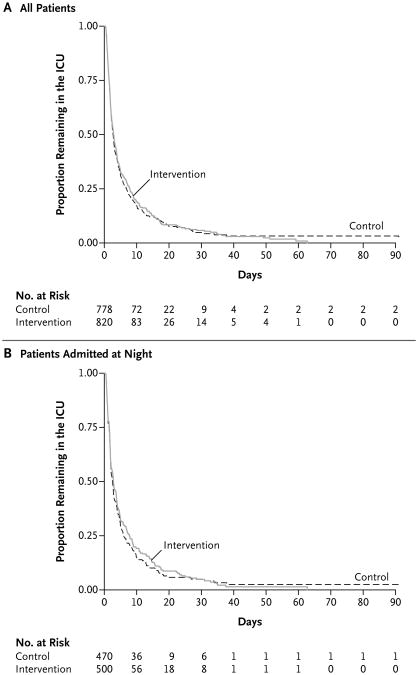
Methods: We conducted a 1-year randomized trial in an academic medical ICU of the effects of nighttime staffing with in-hospital intensivists (intervention) as compared with nighttime coverage by daytime intensivists who were available for consultation by telephone (control). We randomly assigned blocks of 7 consecutive nights to the intervention or the control strategy. The primary outcome was patients' length of stay in the ICU. Secondary outcomes were patients' length of stay in the hospital, ICU and in-hospital mortality, discharge disposition, and rates of readmission to the ICU. For length-of-stay outcomes, we performed time-to-event analyses, with data censored at the time of a patient's death or transfer to another ICU.
Results: A total of 1598 patients were included in the analyses. The median Acute Physiology and Chronic Health Evaluation (APACHE) III score (in which scores range from 0 to 299, with higher scores indicating more severe illness) was 67 (interquartile range, 47 to 91), the median length of stay in the ICU was 52.7 hours (interquartile range, 29.0 to 113.4), and mortality in the ICU was 18%. Patients who were admitted on intervention days were exposed to nighttime intensivists on more nights than were patients admitted on control days (median, 100% of nights [interquartile range, 67 to 100] vs. median, 0% [interquartile range, 0 to 33]; P<0.001). Nonetheless, intensivist staffing on the night of admission did not have a significant effect on the length of stay in the ICU (rate ratio for the time to ICU discharge, 0.98; 95% confidence interval [CI], 0.88 to 1.09; P=0.72), ICU mortality (relative risk, 1.07; 95% CI, 0.90 to 1.28), or any other end point. Analyses restricted to patients who were admitted at night showed similar results, as did sensitivity analyses that used different definitions of exposure and outcome.
Conclusions: In an academic medical ICU in the United States, nighttime in-hospital intensivist staffing did not improve patient outcomes. (Funded by University of Pennsylvania Health System and others; ClinicalTrials.gov number, NCT01434823.).
Figures
Comment in
-
Nighttime physician staffing in an intensive care unit.N Engl J Med. 2013 Sep 12;369(11):1075. doi: 10.1056/NEJMc1308523. N Engl J Med. 2013. PMID: 24024847 No abstract available.
-
Nighttime physician staffing in an intensive care unit.N Engl J Med. 2013 Sep 12;369(11):1074. doi: 10.1056/NEJMc1308523. N Engl J Med. 2013. PMID: 24024848 No abstract available.
-
Nighttime physician staffing in an intensive care unit.N Engl J Med. 2013 Sep 12;369(11):1074. doi: 10.1056/NEJMc1308523. N Engl J Med. 2013. PMID: 24024849 No abstract available.
-
Nighttime physician staffing in an intensive care unit.N Engl J Med. 2013 Sep 12;369(11):1075. doi: 10.1056/NEJMc1308523. N Engl J Med. 2013. PMID: 24024850 No abstract available.
References
-
- Hanson CW, III, Deutschman CS, Anderson HL, III, et al. Effects of an organized critical care service on outcomes and resource utilization: a cohort study. Crit Care Med. 1999;27:270–4. - PubMed
-
- Pronovost PJ, Angus DC, Dorman T, Robinson KA, Dremsizov TT, Young TL. Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review. JAMA. 2002;288:2151–62. - PubMed
-
- Vincent JL. Need for intensivists in intensive-care units. Lancet. 2000;356:695–6. - PubMed
-
- Rubenfeld GD, Angus DC. Are intensivists safe? Ann Intern Med. 2008;148:877–9. - PubMed
-
- Burnham EL, Moss M, Geraci MW. The case for 24/7 in-house intensivist coverage. Am J Respir Crit Care Med. 2010;181:1159–60. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical