

Tissue engineering rib with the incorporation of biodegradable polymer cage and BMSCs/decalcified bone: an experimental study in a canine model
- PMID: 23688344
- PMCID: PMC3695786
- DOI: 10.1186/1749-8090-8-133
Tissue engineering rib with the incorporation of biodegradable polymer cage and BMSCs/decalcified bone: an experimental study in a canine model
Abstract
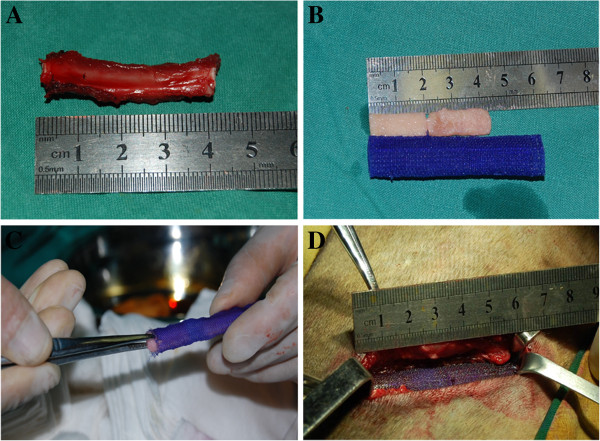
Background: The reconstruction of large bone defects, including rib defects, remains a challenge for surgeons. In this study, we used biodegradable polydioxanone (PDO) cages to tissue engineer ribs for the reconstruction of 4cm-long costal defects.
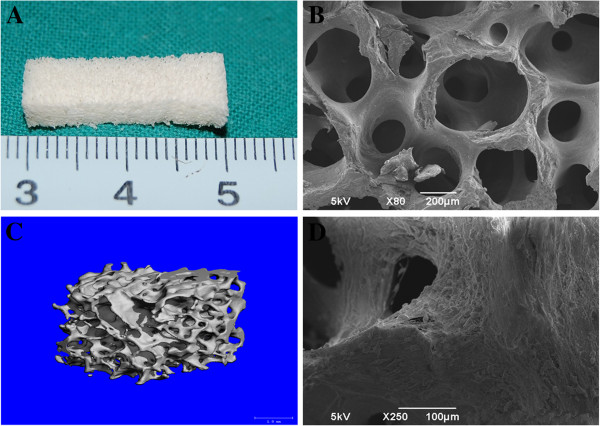
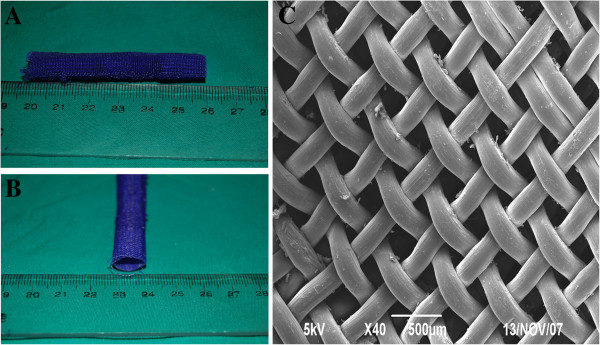
Methods: PDO sutures were used to weave 6cm long and 1cm diameter cages. Demineralized bone matrix (DBM) which is a xenograft was molded into cuboids and seeded with second passage bone marrow mesenchymal stem cells (BMSCs) that had been osteogenically induced. Two DBM cuboids seeded with BMSCs were put into the PDO cage and used to reconstruct the costal defects. Radiographic examination including 3D reconstruction, histologic examination and mechanical test was performed after 24 postoperative weeks.
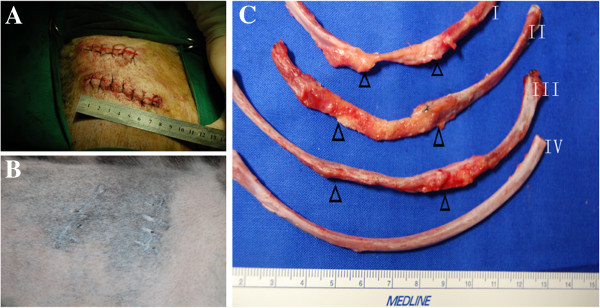
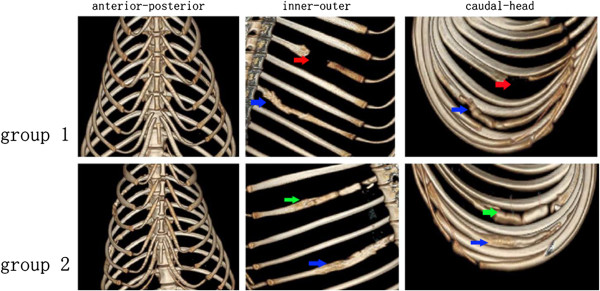
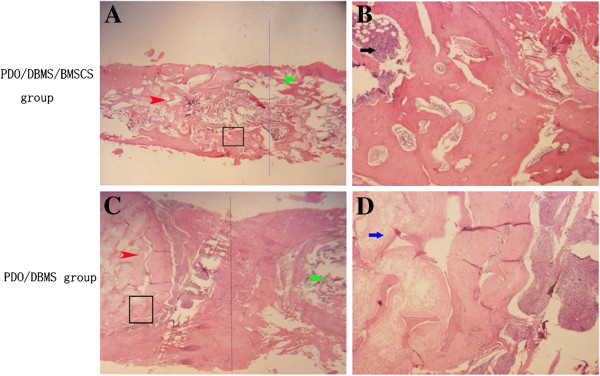
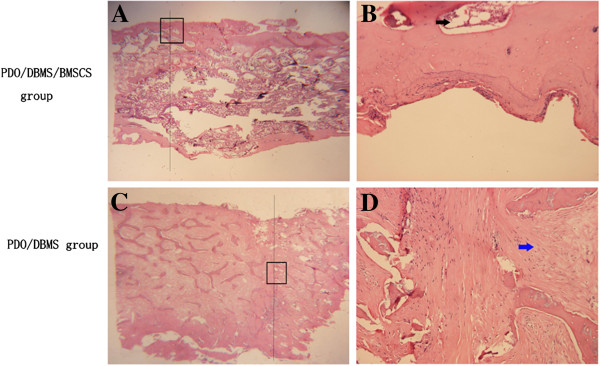
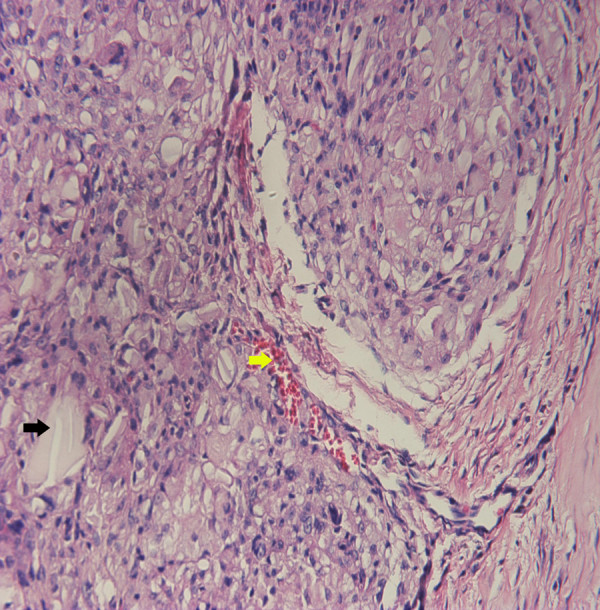
Results: All the experimental subjects survived. In all groups, the PDO cage had completely degraded after 24 weeks and been replaced by fibrous tissue. Better shape and radian were achieved in PDO cages filled with DBM and BMSCs than in the other two groups (cages alone, or cages filled with acellular DBM cuboids). When the repaired ribs were subjected to an outer force, the ribs in the PDO cage/DBMs/BMSCs group kept their original shape while ribs in the other two groups deformed. In the PDO cage/DBMs/BMSCs groups, we also observed bony union at all the construct interfaces while there was no bony union observed in the other two groups. This result was also confirmed by radiographic and histologic examination.
Conclusions: This study demonstrates that biodegradable PDO cage in combination with two short BMSCs/DBM cuboids can repair large rib defects. The satisfactory repair rate suggests that this might be a feasible approach for large bone repair.
Figures
Similar articles
-
Chest wall reconstruction in a canine model using polydioxanone mesh, demineralized bone matrix and bone marrow stromal cells.Biomaterials. 2009 Jul;30(19):3224-33. doi: 10.1016/j.biomaterials.2009.02.007. Epub 2009 Feb 23. Biomaterials. 2009. PMID: 19233465
-
Repair of canine mandibular bone defects with bone marrow stromal cells and coral.Tissue Eng Part A. 2010 Apr;16(4):1385-94. doi: 10.1089/ten.TEA.2009.0472. Tissue Eng Part A. 2010. PMID: 19925049
-
Repair of canine mandibular bone defects with bone marrow stromal cells and porous beta-tricalcium phosphate.Biomaterials. 2007 Feb;28(6):1005-13. doi: 10.1016/j.biomaterials.2006.10.015. Epub 2006 Nov 7. Biomaterials. 2007. PMID: 17092556
-
Restoration of mandibular bone defects with demineralized bone matrix combined with three-dimensional cultured bone marrow-derived mesenchymal stem cells in minipig models.J Mater Sci Mater Med. 2018 Aug 31;29(9):147. doi: 10.1007/s10856-018-6152-3. J Mater Sci Mater Med. 2018. PMID: 30171486
-
Adenovirus-Mediated Expression of BMP-2 and BFGF in Bone Marrow Mesenchymal Stem Cells Combined with Demineralized Bone Matrix For Repair of Femoral Head Osteonecrosis in Beagle Dogs.Cell Physiol Biochem. 2017;43(4):1648-1662. doi: 10.1159/000484026. Epub 2017 Oct 18. Cell Physiol Biochem. 2017. PMID: 29045937
Cited by
-
Three dimensional de novo micro bone marrow and its versatile application in drug screening and regenerative medicine.Exp Biol Med (Maywood). 2015 Aug;240(8):1029-38. doi: 10.1177/1535370215594583. Exp Biol Med (Maywood). 2015. PMID: 26283705 Free PMC article. Review.
-
Repair of bone defects with prefabricated vascularized bone grafts and double-labeled bone marrow-derived mesenchymal stem cells in a rat model.Sci Rep. 2017 Feb 2;7:39431. doi: 10.1038/srep39431. Sci Rep. 2017. PMID: 28150691 Free PMC article.
References
-
- Gupta SS, Singh O, Soni M, Raikwar RS, Mathur RK. Extra-osseous Ewing's sarcoma of chest wall. ANZ J Surg. 2009;79(10):752–753. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
