

Rectal forceps biopsy procedure in cystic fibrosis: technical aspects and patients perspective for clinical trials feasibility
- PMID: 23688510
- PMCID: PMC3679995
- DOI: 10.1186/1471-230X-13-91
Rectal forceps biopsy procedure in cystic fibrosis: technical aspects and patients perspective for clinical trials feasibility
Abstract
Background: Measurements of CFTR function in rectal biopsies ex vivo have been used for diagnosis and prognosis of Cystic Fibrosis (CF) disease. Here, we aimed to evaluate this procedure regarding: i) viability of the rectal specimens obtained by biopsy forceps for ex vivo bioelectrical and biochemical laboratory analyses; and ii) overall assessment (comfort, invasiveness, pain, sedation requirement, etc.) of the rectal forceps biopsy procedure from the patients perspective to assess its feasibility as an outcome measure in clinical trials.
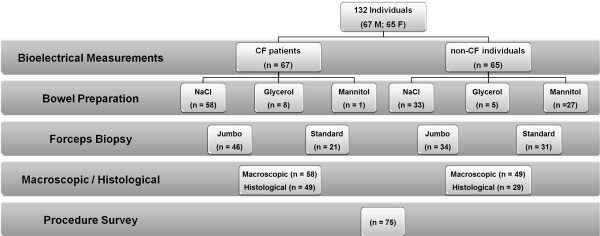
Methods: We compared three bowel preparation solutions (NaCl 0.9%, glycerol 12%, mannitol), and two biopsy forceps (standard and jumbo) in 580 rectal specimens from 132 individuals (CF and non-CF). Assessment of the overall rectal biopsy procedure (obtained by biopsy forceps) by patients was carried out by telephone surveys to 75 individuals who underwent the sigmoidoscopy procedure.
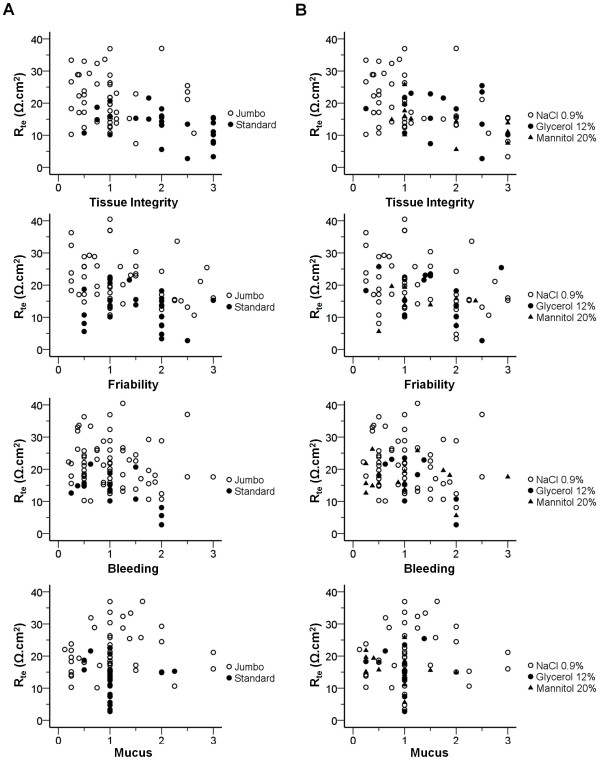
Results: Integrity and friability of the tissue specimens correlate with their transepithelial resistance (r = -0.438 and -0.305, respectively) and are influenced by the bowel preparation solution and biopsy forceps used, being NaCl and jumbo forceps the most compatible methods with the electrophysiological analysis. The great majority of the individuals (76%) did not report major discomfort due to the short procedure time (max 15 min) and considered it relatively painless (79%). Importantly, most (88%) accept repeating it at least for one more time and 53% for more than 4 times.
Conclusions: Obtaining rectal biopsies with a flexible endoscope and jumbo forceps after bowel preparation with NaCl solution is a safe procedure that can be adopted for both adults and children of any age, yielding viable specimens for CFTR bioelectrical/biochemical analyses. The procedure is well tolerated by patients, demonstrating its feasibility as an outcome measure in clinical trials.
Figures
References
-
- Rich DP, Anderson MP, Gregory RJ, Cheng SH, Paul S, Jefferson DM, McCann JD, Klinger KW, Smith AE, Welsh MJ. Expression of cystic fibrosis transmembrane conductance regulator corrects defective chloride channel regulation in cystic fibrosis airway epithelial cells. Nature. 1990;347(6291):358–363. doi: 10.1038/347358a0. - DOI - PubMed
-
- Farrell PM, Rosenstein BJ, White TB, Accurso FJ, Castellani C, Cutting GR, Durie PR, Vicky A, Massie J, Parad RB. Guidelines for Diagnosis of Cystic Fibrosis in Newborns through Older Adults: Cystic Fibrosis Foundation Consensus Report. J Pediatrics. 2008;153(2):S4–S14. doi: 10.1016/j.jpeds.2008.05.005. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
