

Physiological biomarkers of acute kidney injury: a conceptual approach to improving outcomes
- PMID: 23689656
- PMCID: PMC3856226
- DOI: 10.1159/000349967
Physiological biomarkers of acute kidney injury: a conceptual approach to improving outcomes
Abstract
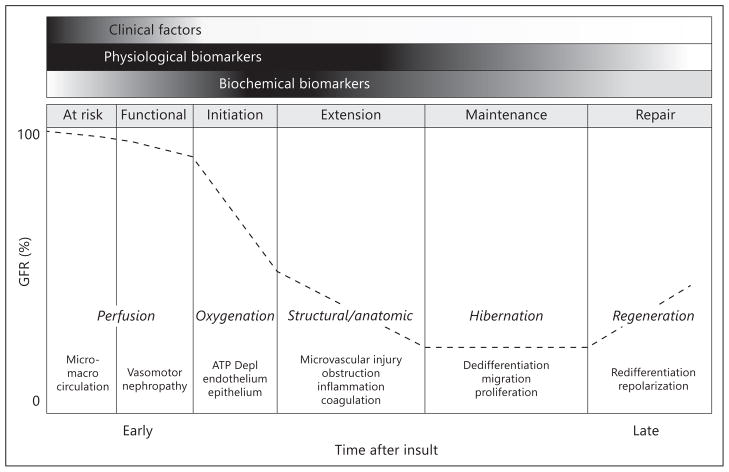
The past 5-10 years have brought significant advances in the identification and validation of novel biochemical biomarkers in the prevention and treatment of acute kidney injury (AKI). These biochemical biomarkers remain research tools but we anticipate that soon they will be employed in clinical practice. A Consensus Conference held by the Acute Dialysis Quality Initiative (ADQI) recently reviewed the evidence, and identified gaps and a research agenda. Furthermore, at this meeting was the birth of an initiative to comprehensively identify new opportunities to characterize the physiological changes during the course of AKI based upon a conceptual framework for the detection and monitoring of renal ischemia-reperfusion injury. This framework includes a transition from monitoring physiological biomarkers of adequate renal perfusion, to pathophysiologic biomarkers of renal hypoperfusion, and finally biomarkers of kidney cell structural injury/damage. Techniques to measure physiological changes in AKI include several physiological variables that might be used in an interactive way to supplement clinical information and biochemical damage biomarkers in the diagnosis and management of AKI. This review summarizes the spectrum of physiological parameters and potential new physiological methods that enable identification of high-risk patients for AKI, facilitate early diagnosis, and differential diagnosis to guide therapeutic management and prognostication. Finally, we propose a research agenda for the next 5 years to facilitate the development and validation of physiological biomarkers in AKI.
Copyright © 2013 S. Karger AG, Basel.
Figures
References
-
- Sutton TA, Fisher CJ, Molitoris BA. Microvascular endothelial injury and dysfunction during ischemic acute renal failure. Kidney Int. 2002;62:1539–1549. - PubMed
-
- Welch WJ. Intrarenal oxygen and hypertension. Clin Exp Pharmacol Physiol. 2006;33:1002–1005. - PubMed
-
- Evans RG, Gardiner BS, Smith DW, O’Connor PM. Intrarenal oxygenation: unique challenges and the biophysical basis of homeostasis. Am J Physiol Renal Physiology. 2008;295:F1259–F1270. - PubMed
-
- Hostetter TH. Human renal response to meat meal. Am J Physiol. 1986;250:F613–F618. - PubMed
-
- Legrand M, Mik EG, Balestra GM, Lutter R, Pirracchio R, Payen D, Ince C. Fluid resuscitation does not improve renal oxygenation during hemorrhagic shock in rats. Anesthesiology. 2010;112:119–127. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
