

Association between a hospital's rate of cardiac arrest incidence and cardiac arrest survival
- PMID: 23689900
- PMCID: PMC4181325
- DOI: 10.1001/jamainternmed.2013.1026
Association between a hospital's rate of cardiac arrest incidence and cardiac arrest survival
Abstract
Importance: National efforts to measure hospital performance in treating cardiac arrest have focused on case survival, with the hope of improving survival after cardiac arrest. However, it is plausible that hospitals with high case-survival rates do a poor job of preventing cardiac arrests in the first place.
Objective: To describe the association between inpatient cardiac arrest incidence and survival rates.
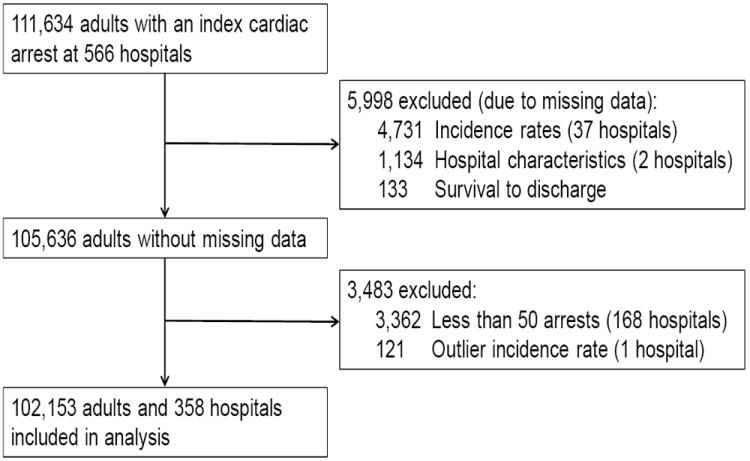
Design: Within a large, national registry, we identified hospitals with at least 50 adult in-hospital cardiac arrest cases between January 1, 2000, and November 30, 2009. We used multivariable hierarchical regression to evaluate the correlation between a hospital's cardiac arrest incidence rate and its case-survival rate after adjusting for patient and hospital characteristics.
Main outcomes and measures: The correlation between a hospital's incidence rate and case-survival rate for cardiac arrest.
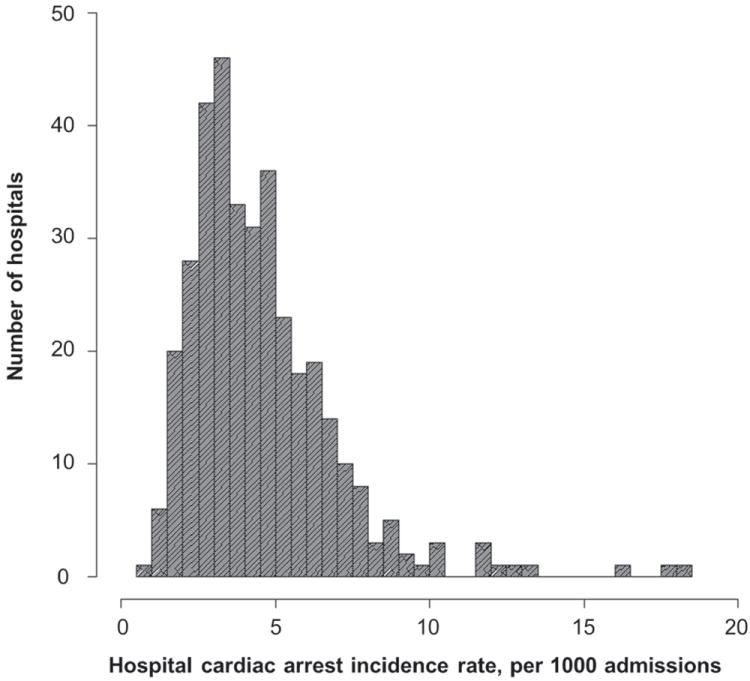
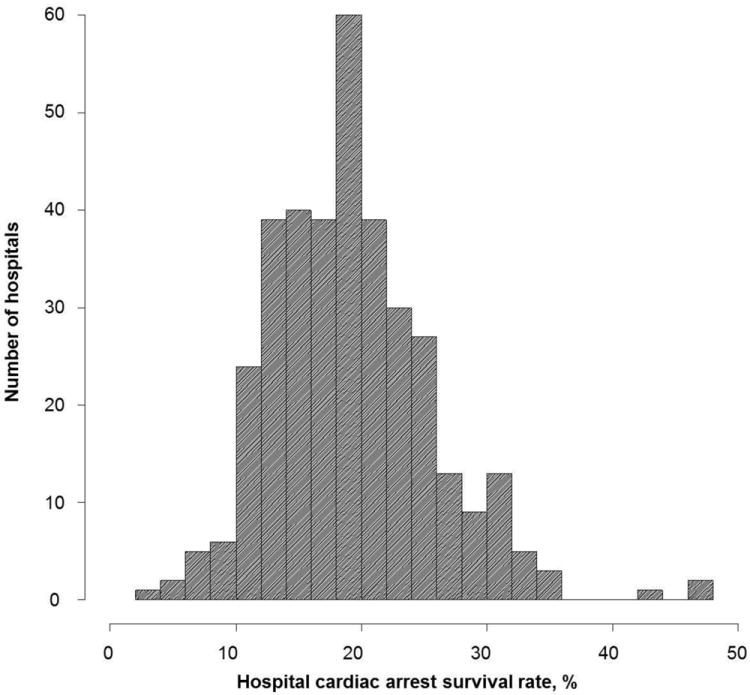
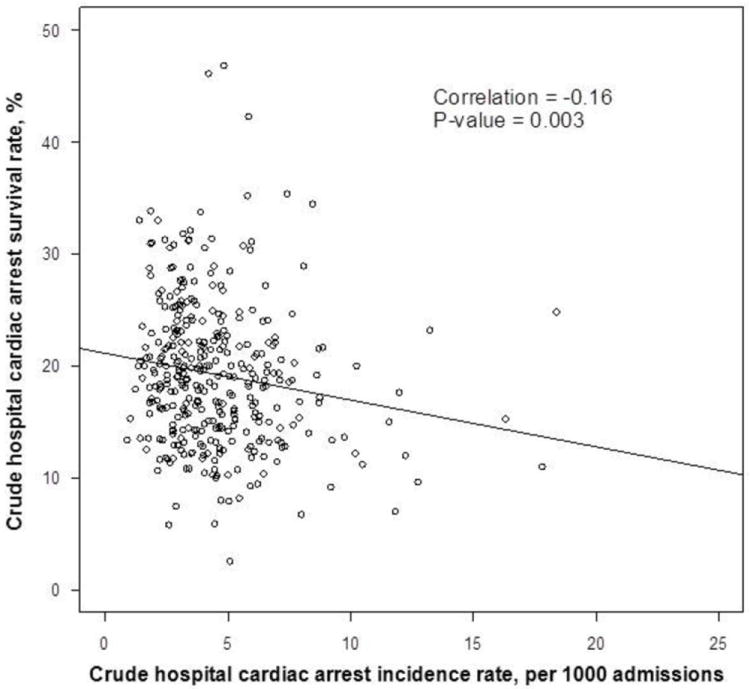
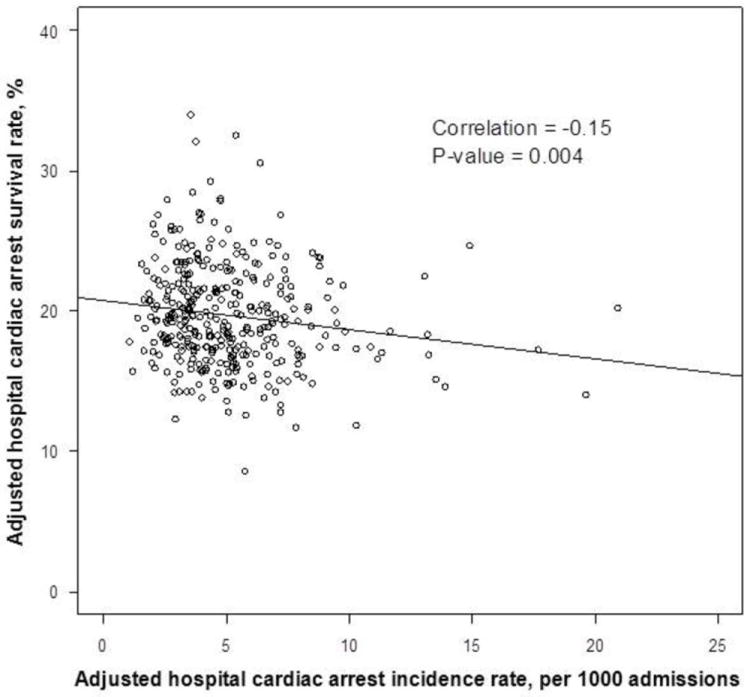
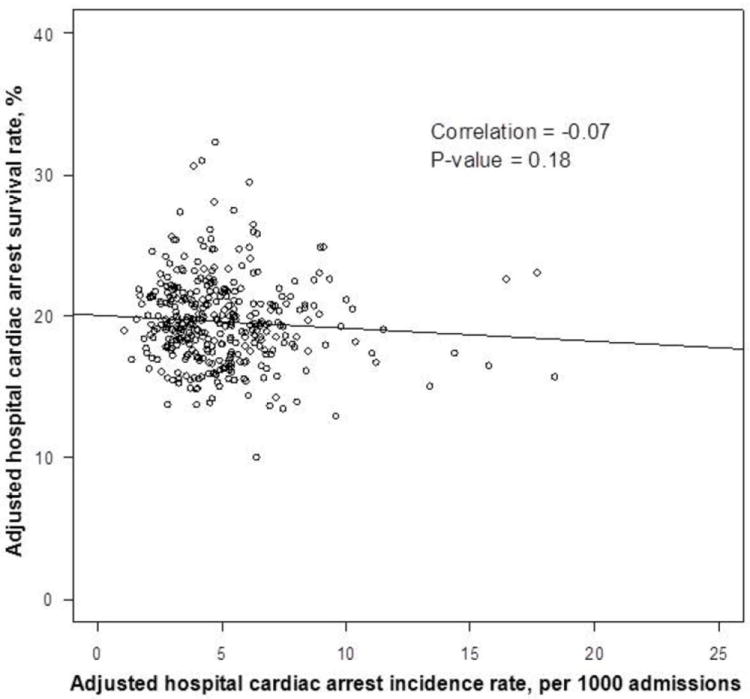
Results: Of 102,153 cases at 358 hospitals, the median hospital cardiac arrest incidence rate was 4.02 per 1000 admissions (interquartile range, 2.95-5.65 per 1000 admissions), and the median hospital case-survival rate was 18.8% (interquartile range, 14.5%-22.6%). In crude analyses, hospitals with higher case-survival rates also had lower cardiac arrest incidence (r, -0.16; P = .003). This relationship persisted after adjusting for patient characteristics (r, -0.15; P = .004). After adjusting for potential mediators of this relationship (ie, hospital characteristics), the relationship between incidence and case survival was attenuated (r, -0.07; P = .18). The one modifiable hospital factor that most attenuated this relationship was a hospital's nurse-to-bed ratio (r, -0.12; P = .03).
Conclusions and relevance: Hospitals with exceptional rates of survival for in-hospital cardiac arrest are also better at preventing cardiac arrests, even after adjusting for patient case mix. This relationship is partially mediated by measured hospital attributes. Performance measures focused on case-survival rates seem an appropriate first step in quality measurement for in-hospital cardiac arrest.
Conflict of interest statement
Figures
References
-
- Brady WJ, Gurka KK, Mehring B, Peberdy MA, O’Connor RE. American Heart Association’s Get with the Guidelines I. In-hospital cardiac arrest: impact of monitoring and witnessed event on patient survival and neurologic status at hospital discharge. Resuscitation. 2011 Jul;82(7):845–852. - PubMed
-
- Chan PS, Krumholz HM, Nichol G, Nallamothu BK. Delayed time to defibrillation after in-hospital cardiac arrest. N Engl J Med. 2008 Jan 3;358(1):9–17. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
