

Optimised z-axis coverage at multidetector-row CT in adults suspected of acute appendicitis
- PMID: 23690436
- PMCID: PMC3745057
- DOI: 10.1259/bjr.20130115
Optimised z-axis coverage at multidetector-row CT in adults suspected of acute appendicitis
Abstract
Objective: To compare diagnostic performances of two reduced z-axis coverages to full coverage of the abdomen and pelvis for the diagnosis of acute appendicitis and alternative diseases at unenhanced CT.
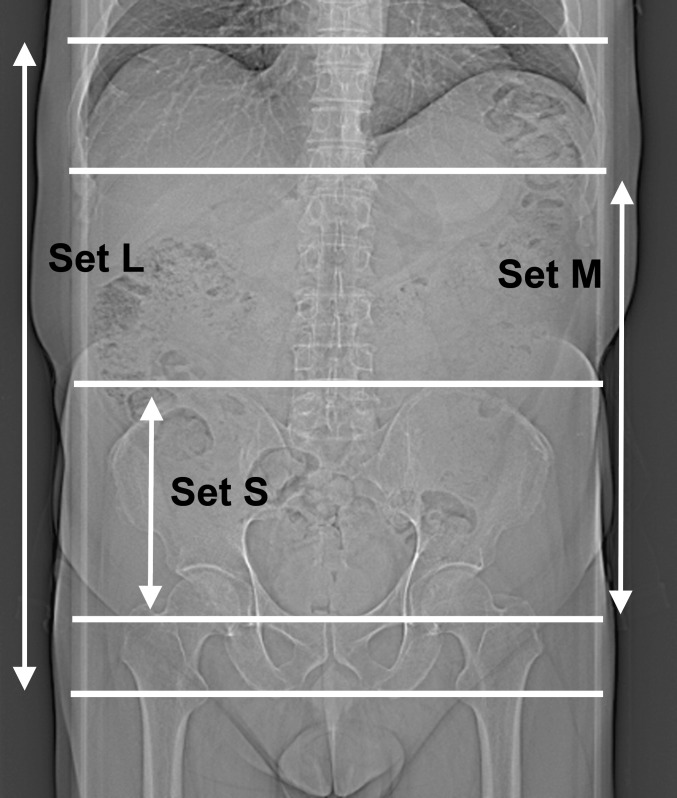
Methods: This study included 152 adults suspected of appendicitis who were enrolled in two ethical committee-approved previous prospective trials. Based on scans covering the entire abdomen and pelvis (set L), two additional sets of images were generated, each with reduced z-axis coverages: (1) from the top of the iliac crests to the pubis (set S) and (2) from the diaphragmatic crus to the pubis (set M). Two readers independently coded the visualisation of the appendix, measured its diameter and proposed a diagnosis (appendicitis or alternative). Final diagnosis was based on surgical findings or clinical follow-up. Fisher exact and McNemar tests and logistic regression were used.
Results: 46 patients had a definite diagnosis of appendicitis and 53 of alternative diseases. The frequency of appendix visualisation was lower for set S than set L for both readers (89% and 84% vs 95% and 91% by Readers A and B, respectively; p=0.021 and 0.022). The probability of giving a correct diagnosis was lower for set S (68%) than set L (78%; odds ratio, 0.611; p=0.008) for both readers, without significant difference between sets L and M (77%, p=0.771); z-axis coverage being reduced by 25% for set M.
Conclusion: Coverage from diaphragmatic crus to pubis, but not focused on pelvis only, can be recommended in adults suspected of appendicitis.
Advances in knowledge: In suspected appendicitis, CT-coverage can be reduced from diaphragmatic crus to pubis.
Figures
References
-
- Birnbaum BA, Wilson SR. Appendicitis at the millennium. Radiology 2000;215:337–48 - PubMed
-
- Johnson PT, Horton KM, Mahesh M, Fishman EK. Multidetector computed tomography for suspected appendicitis: multi-institutional survey of 16-MDCT data acquisition protocols and review of pertinent literature. J Comput Assist Tomogr 2006;30:758–64 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
