

Comorbidities and burden of COPD: a population based case-control study
- PMID: 23691009
- PMCID: PMC3656944
- DOI: 10.1371/journal.pone.0063285
Comorbidities and burden of COPD: a population based case-control study
Abstract
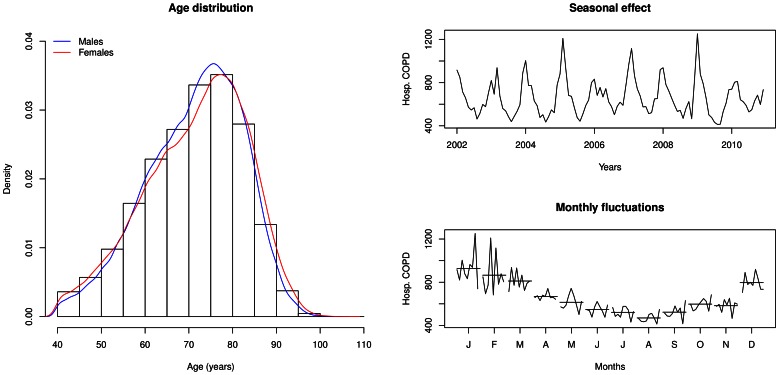
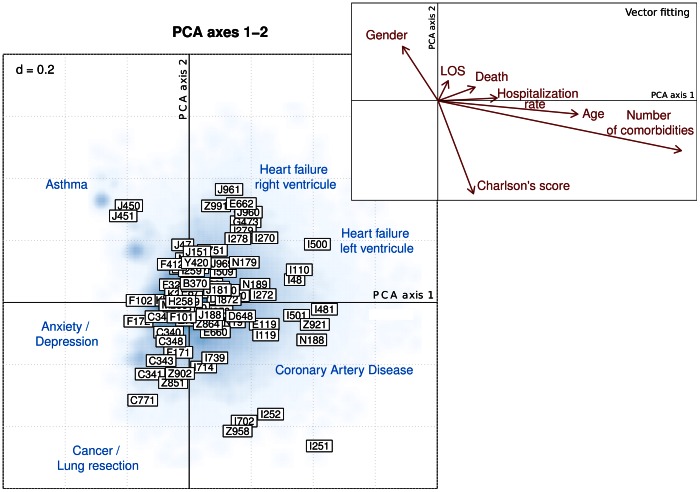
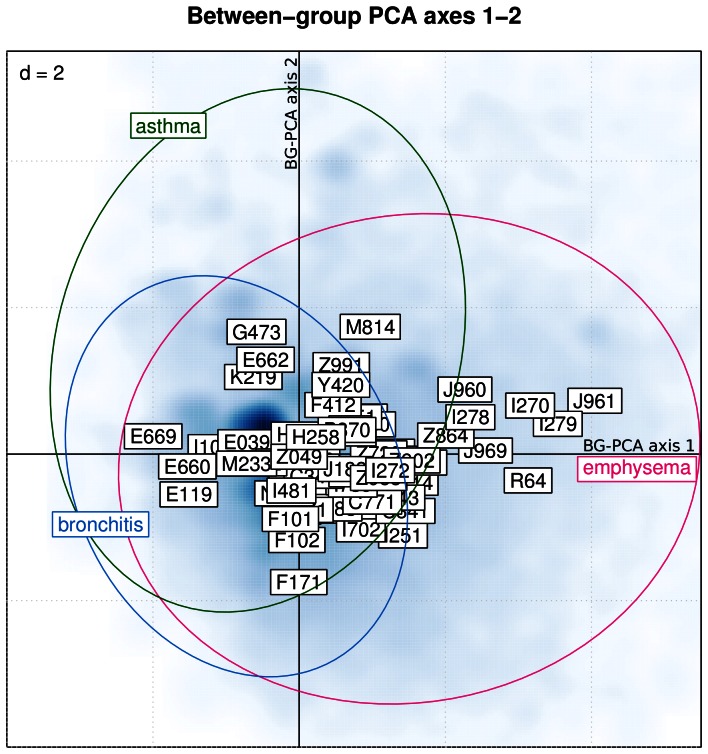
COPD is associated with a relevant burden of disease and a high mortality worldwide. Only recently, the importance of comorbidities of COPD has been recognized. Studies postulated an association with inflammatory conditions potentially sharing pathogenic pathways and worsening overall prognosis. More evidence is required to estimate the role of comorbidities of COPD. Our aim was to investigate the prevalence and clustering of comorbidities associated with COPD, and to estimate their impact on clinically relevant outcomes. In this population-based case-control study, a nation-wide database provided by the Swiss Federal Office for Statistics enclosing every hospital entry covering the years 2002-2010 (n = 12'888'075) was analyzed using MySQL and R statistical software. Statistical methods included non-parametric hypothesis testing by means of Fisher's exact test and Wilcoxon rank sum test, as well as linear models with generalized estimating equation to account for intra-patient variability. Exploratory multivariate approaches were also used for the identification of clusters of comorbidities in COPD patients. In 2.6% (6.3% in patients aged >70 years) of all hospitalization cases an active diagnosis of COPD was recorded. In 21% of these cases, COPD was the main reason for hospitalization. Patients with a diagnosis of COPD had more comorbidities (7 [IQR 4-9] vs. 3 [IQR 1-6]; [Formula: see text]), were more frequently rehospitalized (annual hospitalization rate 0.33 [IQR 0.20-0.67] vs. 0.25 [IQR 0.14-0.43]/year; [Formula: see text]), had a longer hospital stay (9 [IQR 4-15] vs. 5 [IQR 2-11] days; [Formula: see text]), and had higher in-hospital mortality (5.9% [95% CI 5.8%-5.9%] vs. 3.4% [95% CI 3.3%-3.5%]; [Formula: see text]) compared to matched controls. A set of comorbidities was associated with worse outcome. We could identify COPD-related clusters of COPD-comorbidities.
Conflict of interest statement
Figures
References
-
- Vestbo J, Hurd SS, Agusti AG, Jones PW, Vogelmeier C, et al... (2012) Global Strategy for the Diag nosis, Management and Prevention of Chronic Obstructive Pulmonary Disease, GOLD Executive Summary. Am J Respir Crit Care Med : in press. - PubMed
-
- Divo M, Cote C, de Torres JP, Casanova C, Marin JM, et al. (2012) Comorbidities and Risk of Mortality in Patients with Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med 186: 155–161. - PubMed
-
- Patel AR, Hurst JR (2011) Extrapulmonary comorbidities in chronic obstructive pulmonary disease: state of the art. Expert Rev Respir Med 5: 647–662. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
