

The identification of gut neuroendocrine tumor disease by multiple synchronous transcript analysis in blood
- PMID: 23691035
- PMCID: PMC3655166
- DOI: 10.1371/journal.pone.0063364
The identification of gut neuroendocrine tumor disease by multiple synchronous transcript analysis in blood
Abstract
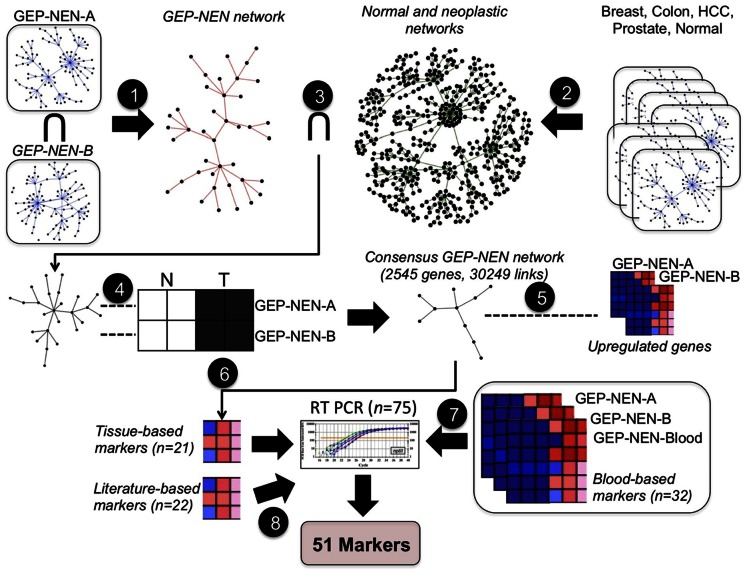
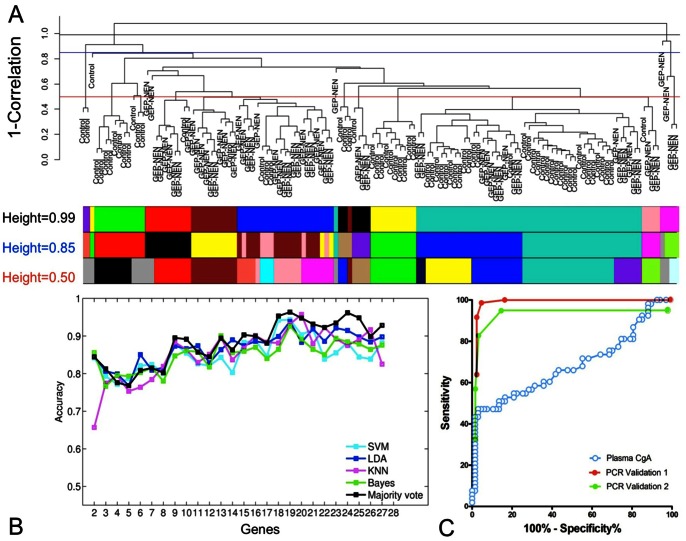
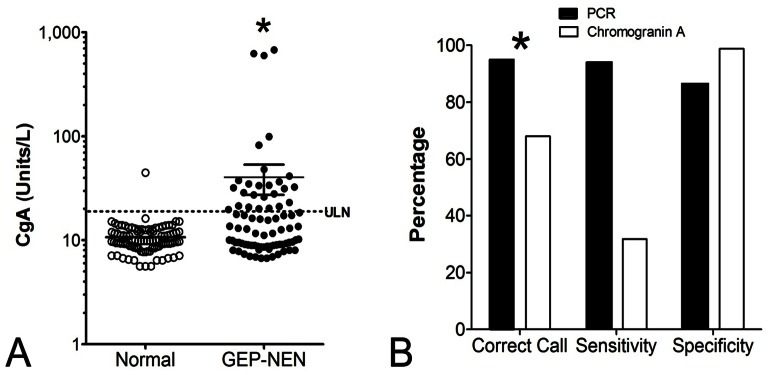
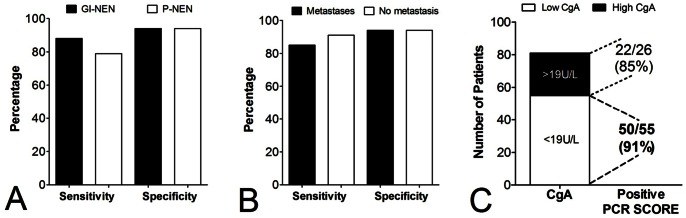
Gastroenteropancreatic (GEP) neuroendocrine neoplasms (NENs) are increasing in both incidence and prevalence. A delay in correct diagnosis is common for these lesions. This reflects the absence of specific blood biomarkers to detect NENs. Measurement of the neuroendocrine secretory peptide Chromogranin A (CgA) is used, but is a single value, is non-specific and assay data are highly variable. To facilitate tumor detection, we developed a multi-transcript molecular signature for PCR-based blood analysis. NEN transcripts were identified by computational analysis of 3 microarray datasets: NEN tissue (n = 15), NEN peripheral blood (n = 7), and adenocarcinoma (n = 363 tumors). The candidate gene signature was examined in 130 blood samples (NENs: n = 63) and validated in two independent sets (Set 1 [n = 115, NENs: n = 72]; Set 2 [n = 120, NENs: n = 58]). Comparison with CgA (ELISA) was undertaken in 176 samples (NENs: n = 81). 51 significantly elevated transcript markers were identified. Gene-based classifiers detected NENs in independent sets with high sensitivity (85-98%), specificity (93-97%), PPV (95-96%) and NPV (87-98%). The AUC for the NEN gene-based classifiers was 0.95-0.98 compared to 0.64 for CgA (Z-statistic 6.97-11.42, p<0.0001). Overall, the gene-based classifier was significantly (χ(2) = 12.3, p<0.0005) more accurate than CgA. In a sub-analysis, pancreatic NENs and gastrointestinal NENs could be identified with similar efficacy (79-88% sensitivity, 94% specificity), as could metastases (85%). In patients with low CgA, 91% exhibited elevated transcript markers. A panel of 51 marker genes differentiates NENs from controls with a high PPV and NPV (>90%), identifies pancreatic and gastrointestinal NENs with similar efficacy, and confirms GEP-NENs when CgA levels are low. The panel is significantly more accurate than the CgA assay. This reflects its utility to identify multiple diverse biological components of NENs. Application of this sensitive and specific PCR-based blood test to NENs will allow accurate detection of disease, and potentially define disease progress enabling monitoring of treatment efficacy.
Conflict of interest statement
Figures
References
-
- Modlin IM, Oberg K, Chung DC, Jensen RT, de Herder WW, et al. (2008) Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol 9: 61–72. - PubMed
-
- Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, et al. (2008) One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol 26: 3063–3072. - PubMed
-
- Yao JC, Pavel M, Phan AT, Kulke MH, Hoosen S, et al. (2011) Chromogranin A and neuron-specific enolase as prognostic markers in patients with advanced pNET treated with everolimus. J Clin Endocrinol Metab 96: 3741–3749. Epub 2011 Oct 3712. - PubMed
-
- AACC (2010) Chromogranin A. Lab Tests Online: American Association for Clinical Chemistry. pp. Details regarding Chromogranin A as a test.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
