

Trends in the prevalence of tuberous sclerosis complex manifestations: an epidemiological study of 166 Japanese patients
- PMID: 23691114
- PMCID: PMC3656843
- DOI: 10.1371/journal.pone.0063910
Trends in the prevalence of tuberous sclerosis complex manifestations: an epidemiological study of 166 Japanese patients
Abstract
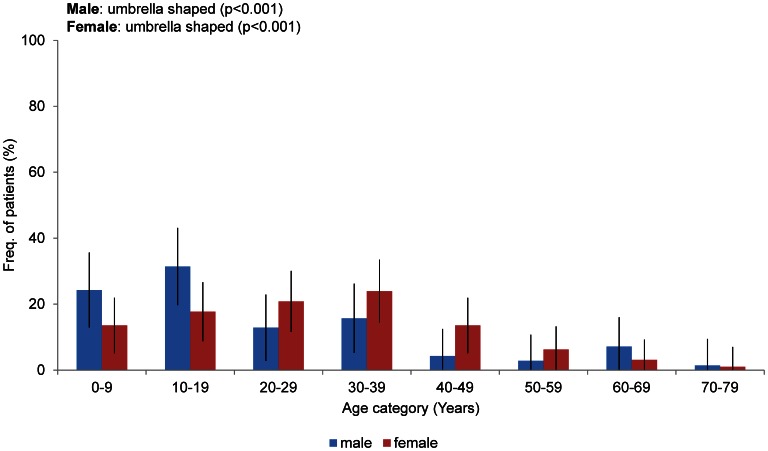
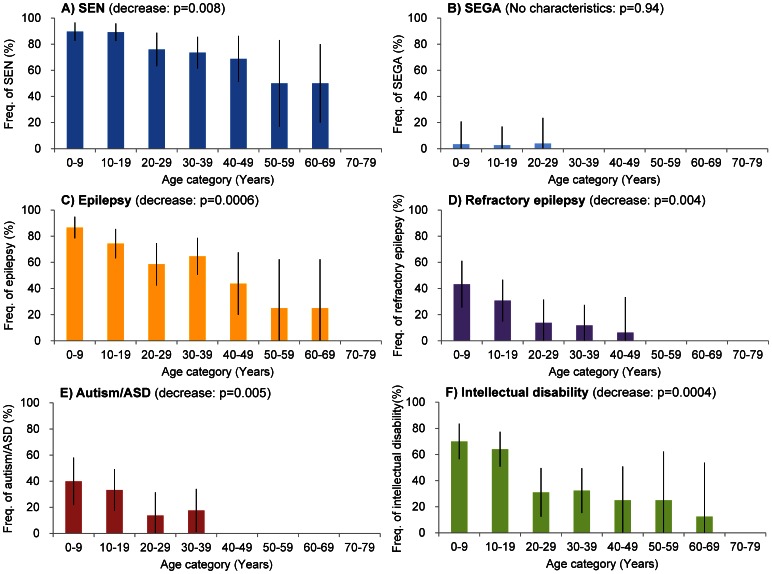
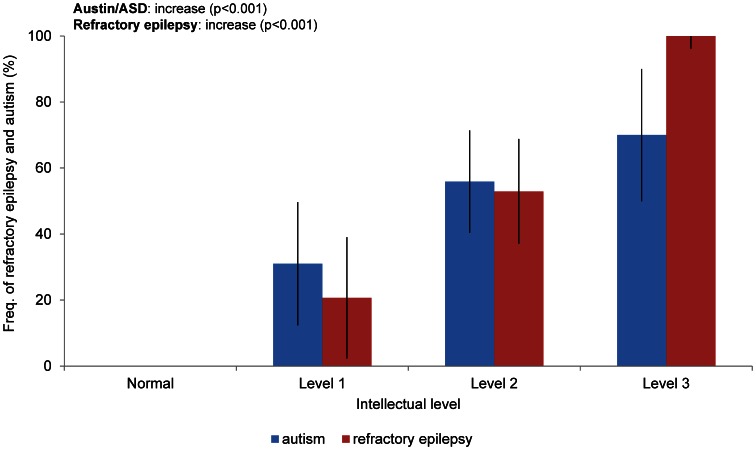
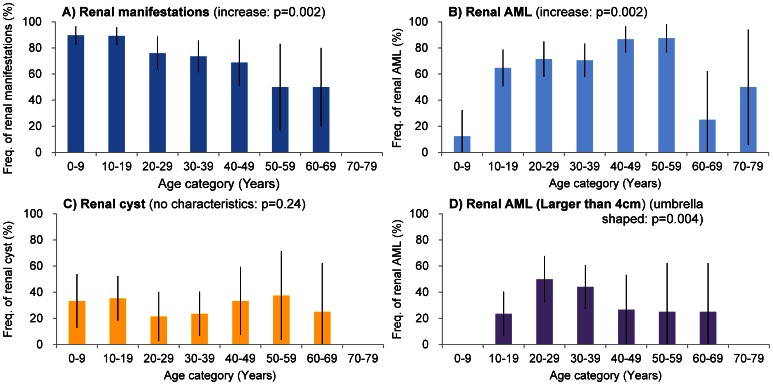
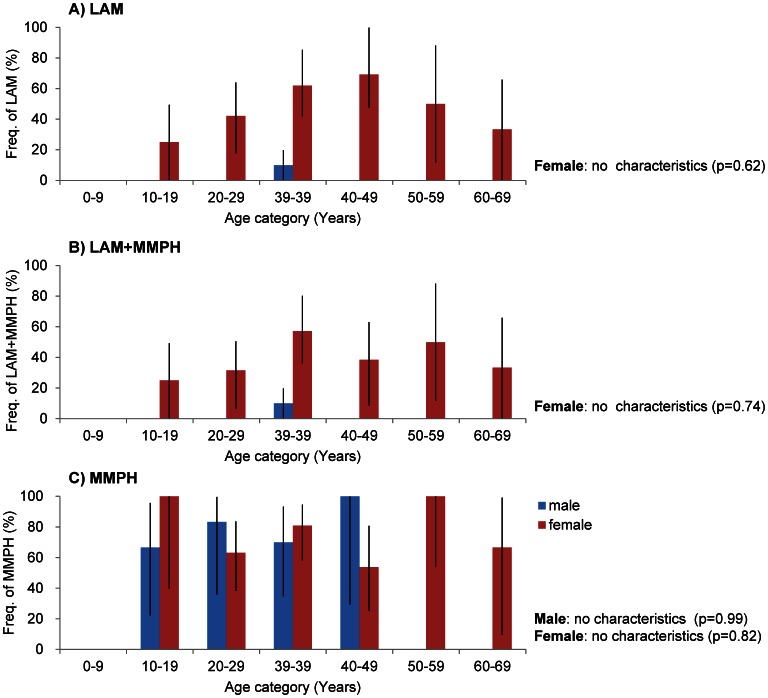
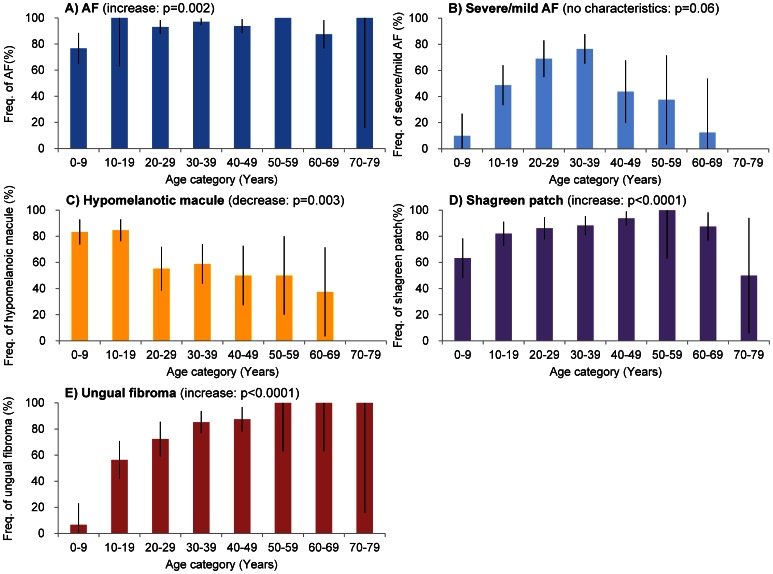
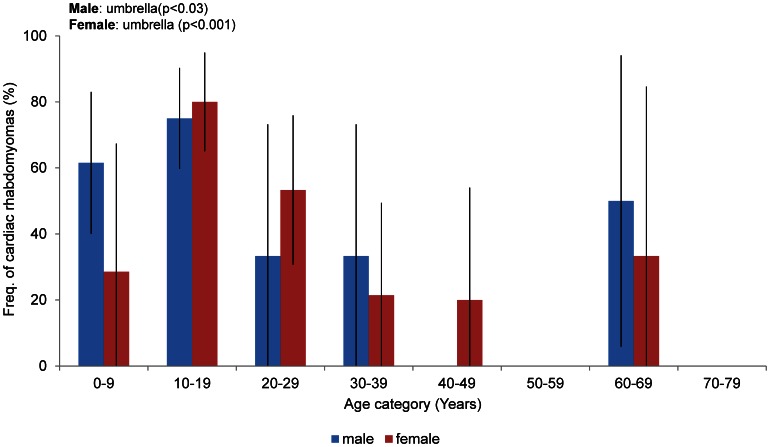
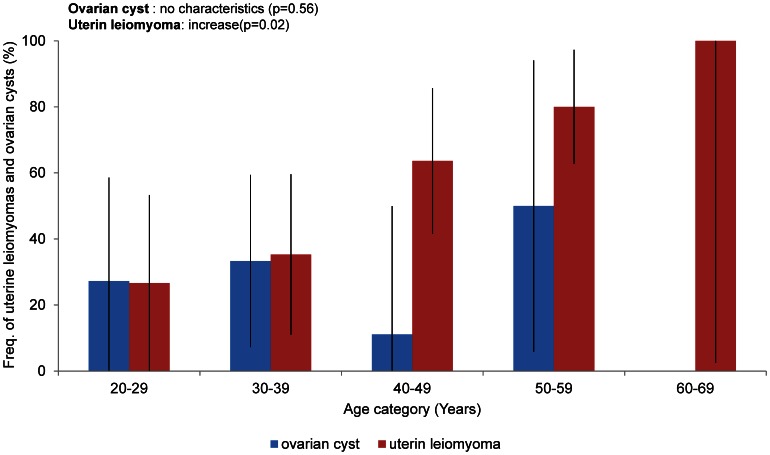
Tuberous sclerosis complex (TSC) is an autosomal dominant disorder with multi-system involvement and variable manifestations. There has been significant progress in TSC research and the development of technologies used to diagnose this disorder. As a result, individuals with mild TSC are now being diagnosed, including many older adults who have not developed seizures or cognitive abnormalities. We conducted a statistical analysis of the frequency of TSC manifestations in a population of Japanese adults and children, comparing our findings with historical data. The chi-square test was used to examine the frequency of each manifestation by age. A total of 166 outpatients at the Department of Dermatology of Osaka University Hospital during the period from January 2001 to March 2011 were included in the study. Compared to previous reports, the frequency of neurologic manifestations (excepting autism) was lower in this cohort, and the frequency of skin manifestations (excepting hypomelanotic macules) was higher in this cohort. The frequencies of pulmonary lymphangioleiomyomatosis and renal manifestations were not significantly different from those previously reported. Regarding the association of each manifestation with age, the frequency of neurologic manifestations (excepting subependymal giant cell astrocytoma) was significantly higher in younger patients than in older patients. The frequency of skin manifestations and renal angiomyolipoma were significantly higher in older patients than in younger patients. Because of their high frequency and visibility, skin manifestations are useful in the diagnosis of TSC. Moreover, uterine perivascular epithelioid cell tumor was also characterized as a new findings associated with TSC.
Conflict of interest statement
Figures
References
-
- Osborne JP, Jones AC, Burley MW, Jeganathan D, Young J, et al. (2000) Non-penetrance in tuberous sclerosis. Lancet 355: 1698. - PubMed
-
- van Slegtenhorst M, de Hoogt R, Hermans C, Nellist M, Janssen B, et al. (1997) Identification of the tuberous sclerosis gene TSC1 on chromosome 9q34. Science 277: 805–808. - PubMed
-
- Identification and characterization of the tuberous sclerosis gene on chromosome 16. Cell 75: 1305–1315. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
