

Completeness and diagnostic validity of recording acute myocardial infarction events in primary care, hospital care, disease registry, and national mortality records: cohort study
- PMID: 23692896
- PMCID: PMC3898411
- DOI: 10.1136/bmj.f2350
Completeness and diagnostic validity of recording acute myocardial infarction events in primary care, hospital care, disease registry, and national mortality records: cohort study
Abstract
Objective: To determine the completeness and diagnostic validity of myocardial infarction recording across four national health record sources in primary care, hospital care, a disease registry, and mortality register.
Design: Cohort study.
Participants: 21 482 patients with acute myocardial infarction in England between January 2003 and March 2009, identified in four prospectively collected, linked electronic health record sources: Clinical Practice Research Datalink (primary care data), Hospital Episode Statistics (hospital admissions), the disease registry MINAP (Myocardial Ischaemia National Audit Project), and the Office for National Statistics mortality register (cause specific mortality data).
Setting: One country (England) with one health system (the National Health Service).
Main outcome measures: Recording of acute myocardial infarction, incidence, all cause mortality within one year of acute myocardial infarction, and diagnostic validity of acute myocardial infarction compared with electrocardiographic and troponin findings in the disease registry (gold standard).
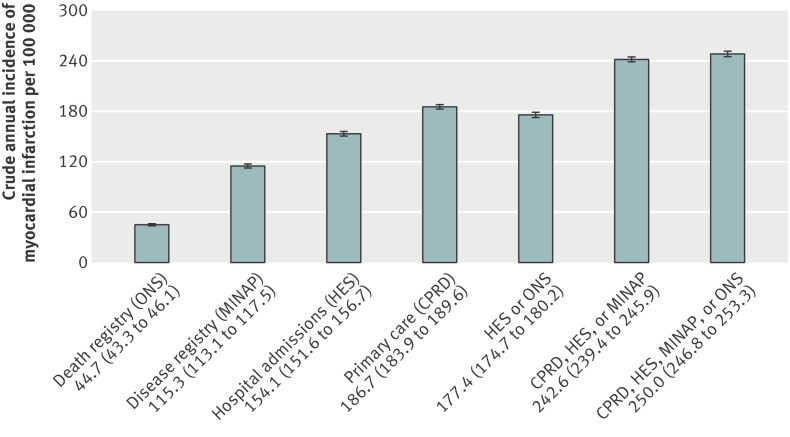
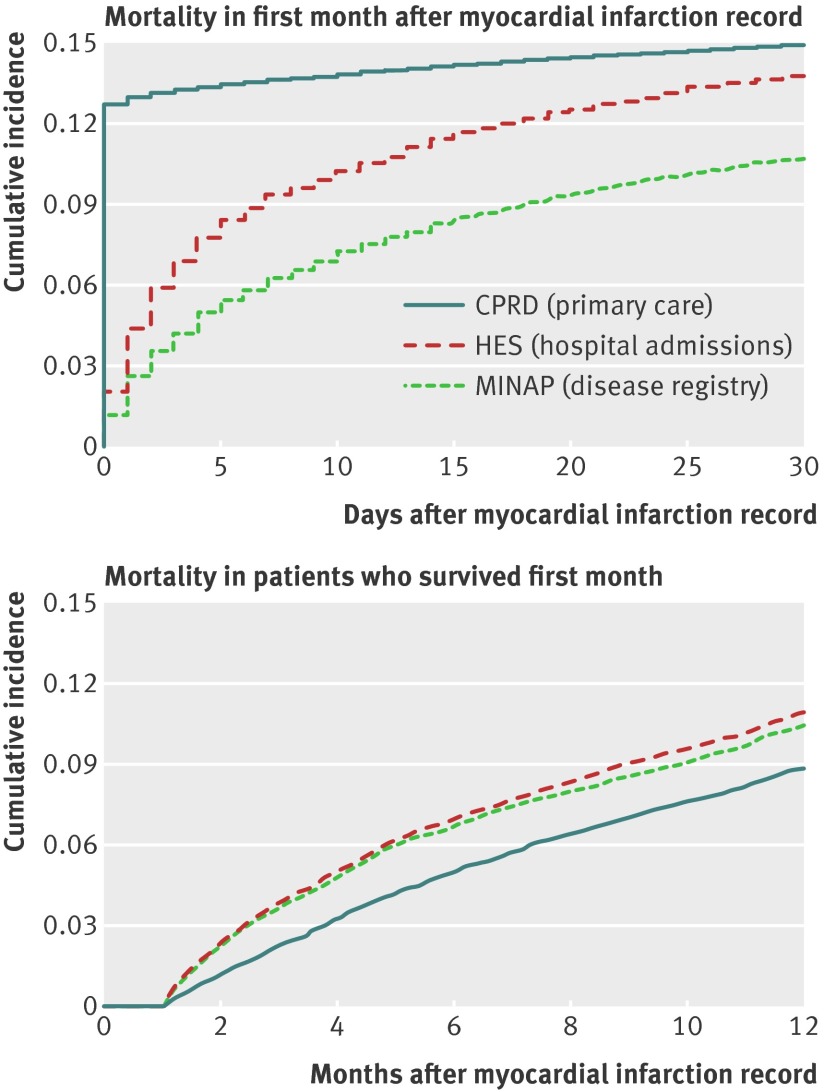
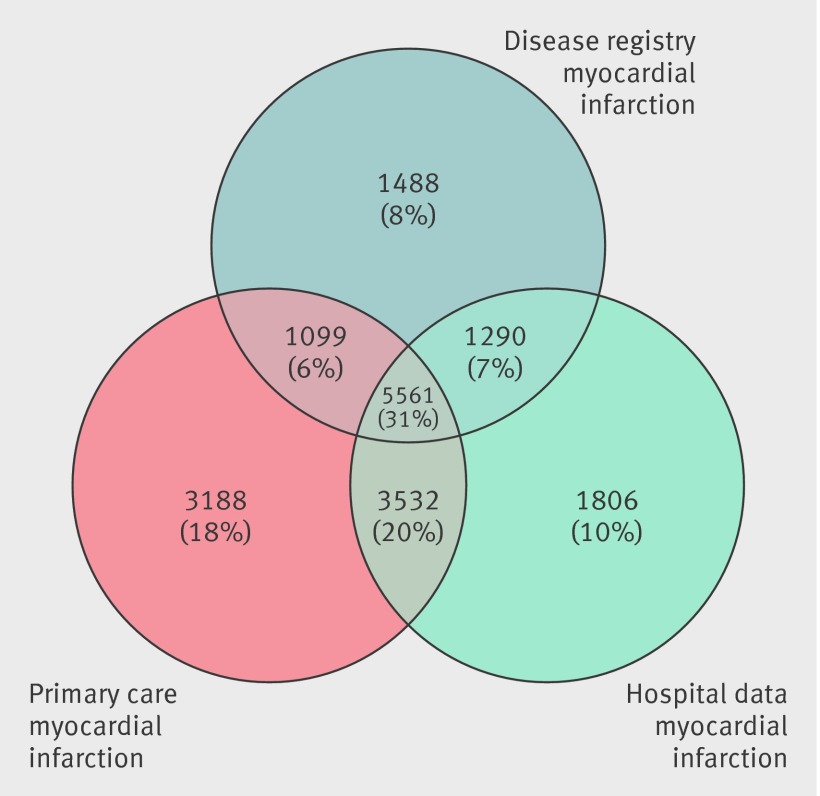
Results: Risk factors and non-cardiovascular coexisting conditions were similar across patients identified in primary care, hospital admission, and registry sources. Immediate all cause mortality was highest among patients with acute myocardial infarction recorded in primary care, which (unlike hospital admission and disease registry sources) included patients who did not reach hospital, but at one year mortality rates in cohorts from each source were similar. 5561 (31.0%) patients with non-fatal acute myocardial infarction were recorded in all three sources and 11 482 (63.9%) in at least two sources. The crude incidence of acute myocardial infarction was underestimated by 25-50% using one source compared with using all three sources. Compared with acute myocardial infarction defined in the disease registry, the positive predictive value of acute myocardial infarction recorded in primary care was 92.2% (95% confidence interval 91.6% to 92.8%) and in hospital admissions was 91.5% (90.8% to 92.1%).
Conclusion: Each data source missed a substantial proportion (25-50%) of myocardial infarction events. Failure to use linked electronic health records from primary care, hospital care, disease registry, and death certificates may lead to biased estimates of the incidence and outcome of myocardial infarction.
Trial registration: NCT01569139 clinicaltrials.gov.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Unlinked data sources underestimate risk of cardiovascular disease.BMJ. 2013 Jun 11;346:f3737. doi: 10.1136/bmj.f3737. BMJ. 2013. PMID: 23757749 No abstract available.
-
Authors' reply to Stevens and McManus.BMJ. 2013 Jun 11;346:f3741. doi: 10.1136/bmj.f3741. BMJ. 2013. PMID: 23757750 No abstract available.
References
-
- The West of Scotland Coronary Prevention Study Group. Computerised record linkage: compared with traditional patient follow-up methods in clinical trials and illustrated in a prospective epidemiological study. J Clin Epidemiol 1995;48:1441-52. - PubMed
-
- Ford I, Murray H, Packard CJ, Shepherd J, Macfarlane PW, Cobbe SM. Long-term follow-up of the west of Scotland coronary prevention study. N Engl J Med 2007;357:1477-86. - PubMed
-
- Collins R. What makes UK Biobank special? Lancet 2012;379:1173-4. - PubMed
-
- Lewsey JD, Leyland AH, Murray GD, Boddy FA. Using routine data to complement and enhance the results of randomised controlled trials. Health Technol Assess 2000;4:1-55. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical