

Genotypic diversity and mixed infection in newborn disease and hearing loss in congenital cytomegalovirus infection
- PMID: 23694837
- PMCID: PMC3785554
- DOI: 10.1097/INF.0b013e31829bb0b9
Genotypic diversity and mixed infection in newborn disease and hearing loss in congenital cytomegalovirus infection
Abstract
Background: Congenital cytomegalovirus (cCMV) is a common congenital infection and a leading nongenetic cause of sensorineural hearing loss (SNHL). CMV exhibits extensive genetic variability, and infection with multiple CMV strains (mixed infection) was shown to be common in congenital CMV. The role of mixed infections in disease and outcome remains to be defined.
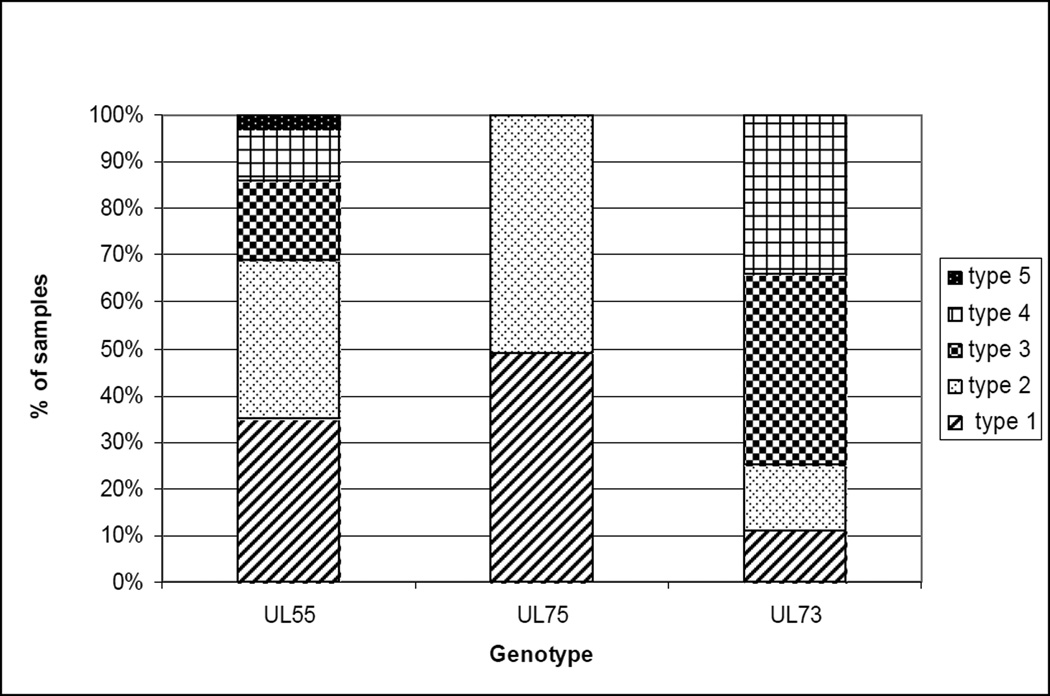
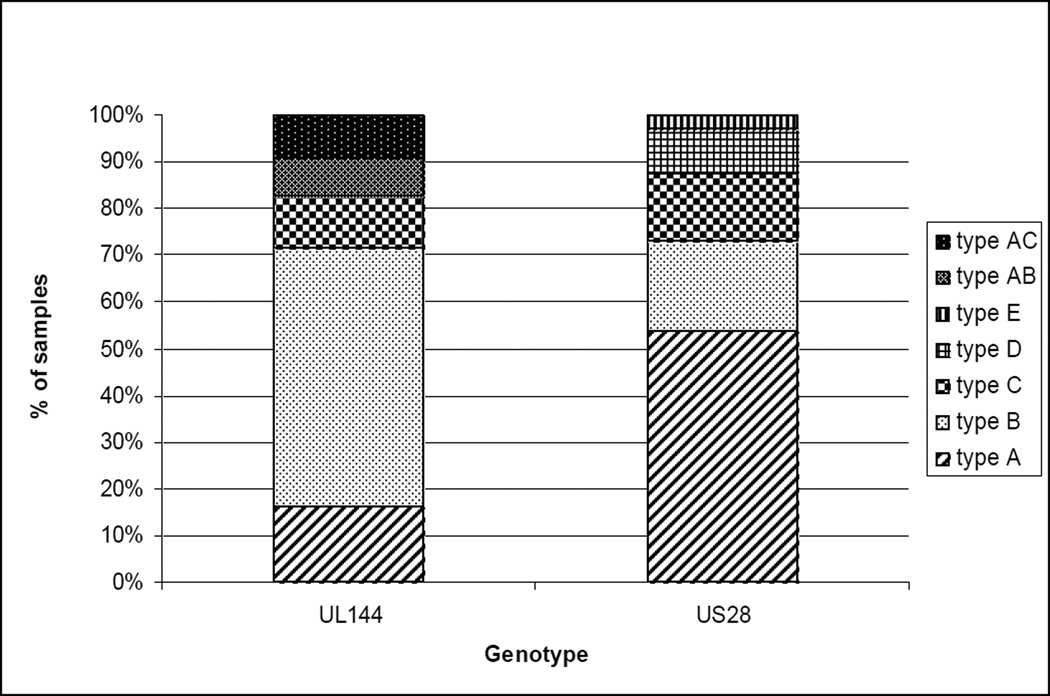
Methods: Genotyping of envelope glycoproteins, UL55 (gB), UL73 (gN) and UL75 (gH), was performed on saliva specimens of 79 infants from the ongoing CMV and Hearing Multicenter Screening (CHIMES) Study and on blood and urine specimens of 52 infants who participated in natural history studies at the University of Alabama at Birmingham. Genotyping of UL144 and US28 was also performed in the CHIMES cohort. The association of individual genotypes and mixed infection with clinical findings at birth and SNHL was examined.
Results: Thirty-seven of 131 infants (28%) were symptomatic at birth and 26 (20%) had SNHL at birth. All known genotypes of UL55, UL75, UL73 and US28 were represented, and no particular genotype was associated with symptomatic infection or SNHL. UL144 subtype C was more common in symptomatic infants but not associated with SNHL. Mixed infection was observed in 59 infants (45%) and not associated with symptoms (P = 0.43) or SNHL at birth (P = 0.82). In the cohort of 52 infants with long-term hearing outcome, mixed infection at birth was not predictive of SNHL.
Conclusions: Mixed infection is common in infants with congenital CMV but is neither associated with symptomatic infection nor associated with SNHL.
Conflict of interest statement
Figures
References
-
- Morton CC, Nance WE. Newborn hearing screening--a silent revolution. N Engl J Med. 2006;354:2151–2164. - PubMed
-
- Dahle AJ, Fowler KB, Wright JD, Boppana SB, Britt WJ, Pass RF. Longitudinal investigations of hearing disorders in children with congenital cytomegalovirus. J Am Acad Audiol. 2000;11:283–290. - PubMed
-
- Britt WJ. Cytomegalovirus. In: Reminghton JS, Klein JO, Wilson CB, Nizet V, Maldonaldo Y, editors. Infectious Diseases of the Fetus and Newborn Infant. 7th ed. Philadelphia: Elsevier Saunders; 2011. pp. 706–755.
-
- Chou SW. Differentiation of cytomegalovirus strains by restriction analysis of DNA sequences amplified from clinical specimens. J Infect Dis. 1990;162:738–742. - PubMed
-
- Coaquette A, Bourgeois A, Dirand C, Varin A, Chen W, Herbein G. Mixed cytomegalovirus glycoprotein B genotypes in immunocompromised patients. Clin Infect Dis. 2004;39:155–161. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
