

Major burn injury is not associated with acute traumatic coagulopathy
- PMID: 23694874
- PMCID: PMC4342258
- DOI: 10.1097/TA.0b013e3182923193
Major burn injury is not associated with acute traumatic coagulopathy
Abstract
Background: The pathophysiology and time course of coagulopathy after major burns are inadequately understood. Our study objectives were to determine whether acute traumatic coagulopathy (ATC) is seen in burn patients at admission and to determine the changes in international normalized ratio (INR), activated partial thromboplastin time (aPTT), platelet count (PLT), and hemoglobin (Hgb) in the first 7 days after injury.
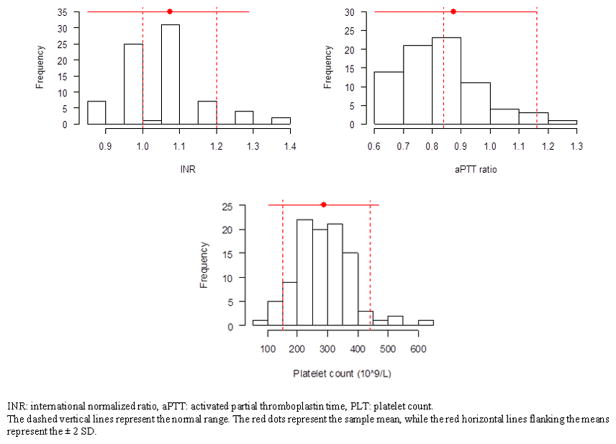
Methods: We conducted a retrospective study of patients with burn injury of at least 15% total body surface area who presented to the University of North Carolina. Data on patient demographics, injury characteristics, and laboratory data (INR, aPTT, PLT, and Hgb) at admission and within the first 7 days after injury were recorded. We defined ATC as INR of 1.3 or greater, aPTT of 1.5 or greater times the mean normal limit, and normal PLT at admission.
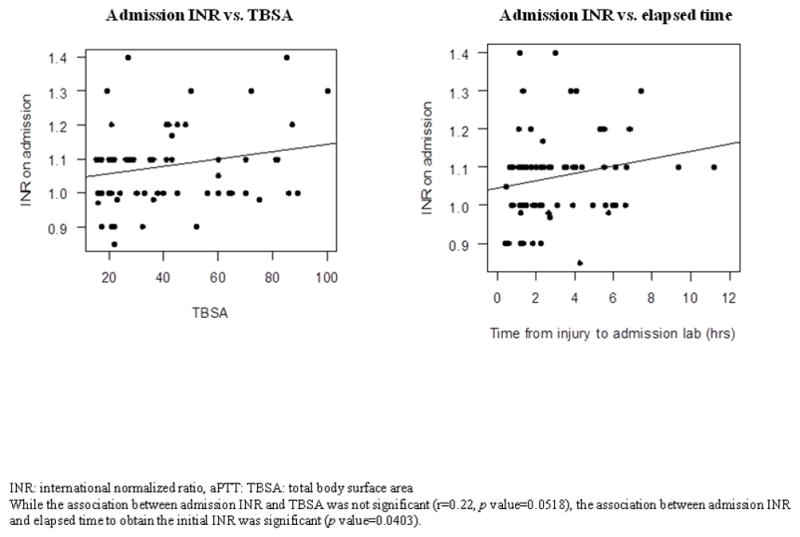
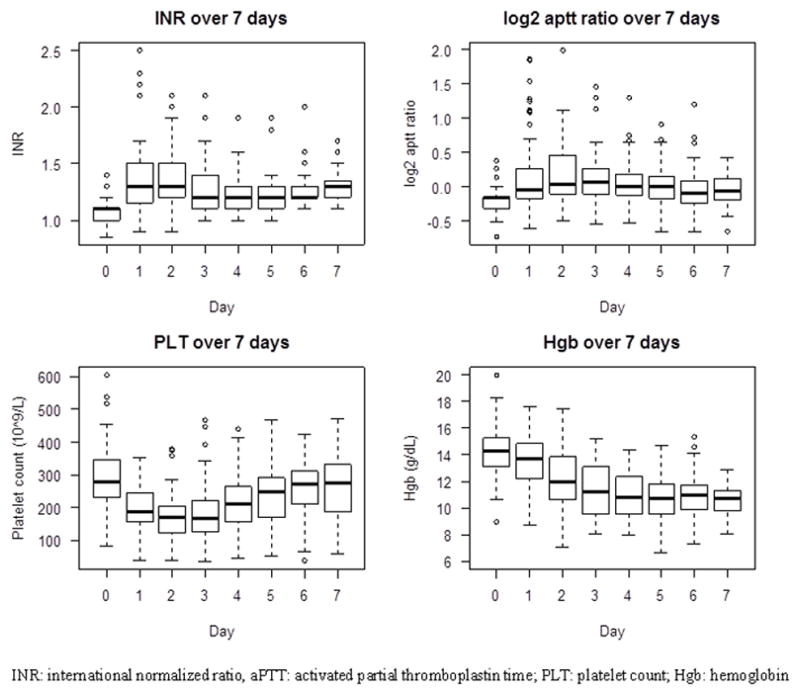
Results: We studied the hematologic profile of 102 patients with burn injury of 15% to 100% total body surface area but did not identify a single patient with ATC at admission. The screening hematologic profile at admission was not influenced by burn severity. In the first 7 days after injury, the INR and aPTT were relatively preserved, while the PLT quickly recovered to baseline after an early decline and the Hgb remained stable at around 10 g/dL; all these changes occurred during the time when the burn patients had received large amounts of fluid resuscitation.
Conclusion: The screening hematologic profile of burn patients at admission is normal, and the standard screening assays do not suggest the existence of ATC at admission. While this is a relatively small study, it provides evidence to suggest that ATC is unique to trauma patients.
Level of evidence: Prognostic study, level III.
Conflict of interest statement
Conflict of Interest:
DMM reported no conflict of interest with this submission but has relevant financial activities outside of this work. For the remaining authors, no conflicts were declared.
Figures
Comment in
-
Major burn injuries and early coagulation dysfunction.J Trauma Acute Care Surg. 2013 Oct;75(4):746-7. doi: 10.1097/01.ta.0000436144.32009.1c. J Trauma Acute Care Surg. 2013. PMID: 24064897 No abstract available.
References
-
- MacLeod JB, Lynn M, McKenney MG, Cohn SM, Murtha M. Early coagulopathy predicts mortality in trauma. J Trauma. 2003;55(1):39–44. - PubMed
-
- Brohi K, Singh J, Heron M, Coats T. Acute Traumatic Coagulopathy. J Trauma. 2003;54(6):1127–30. - PubMed
-
- Maegele M, Lefering R, Yucel N, Tjardes T, Rixen D, Paffrath T, Simanski C, Neugebauer E, Bouillon B AG Polytrauma of the German Trauma Society (DGU) Early coagulopathy in multiple injury: an analysis from the German Trauma Registry on 8724 patients. Injury. 2007;38(3):298–304. - PubMed
-
- Brohi K, Cohen MJ, Ganter MT, Schultz MJ, Levi M, Mackersie RC, Pittet JF. Acute coagulopathy of trauma: hypoperfusion induces systemic anticoagulation and hyperfibrinolysis. J Trauma. 2008;64(5):1211–1217. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
