

Increased perioperative b-type natriuretic peptide associates with heart failure hospitalization or heart failure death after coronary artery bypass graft surgery
- PMID: 23695172
- PMCID: PMC3840806
- DOI: 10.1097/ALN.0b013e318299969c
Increased perioperative b-type natriuretic peptide associates with heart failure hospitalization or heart failure death after coronary artery bypass graft surgery
Abstract
Background: Heart failure (HF) is a leading cause of hospitalization and mortality. Plasma B-type natriuretic peptide (BNP) is an established diagnostic and prognostic ambulatory HF biomarker. We hypothesized that increased perioperative BNP independently associates with HF hospitalization or HF death up to 5 yr after coronary artery bypass graft surgery.
Methods: The authors conducted a two-institution, prospective, observational study of 1,025 subjects (mean age = 64 ± 10 yr SD) undergoing isolated primary coronary artery bypass graft surgery with cardiopulmonary bypass. Plasma BNP was measured preoperatively and on postoperative days 1-5. The study outcome was hospitalization or death from HF, with HF events confirmed by reviewing hospital and death records. Cox proportional hazards analyses were performed with multivariable adjustments for clinical risk factors. Preoperative and peak postoperative BNP were added to the multivariable clinical model in order to assess additional predictive benefit.
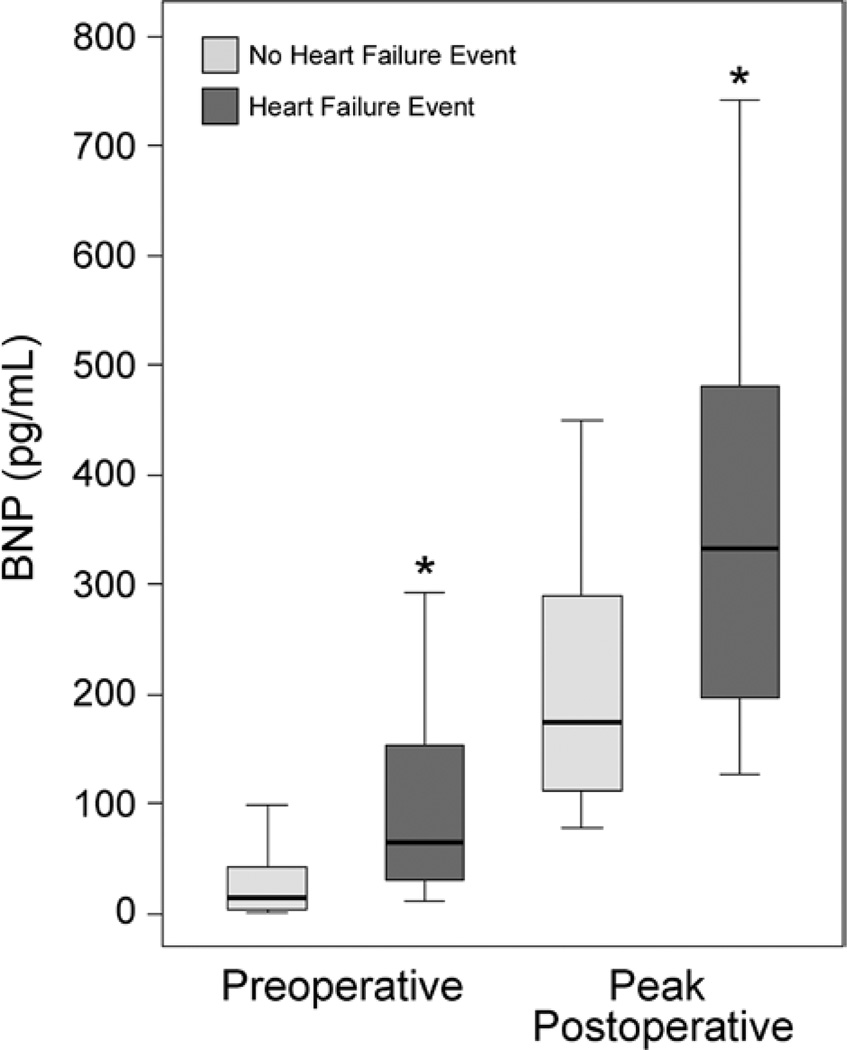
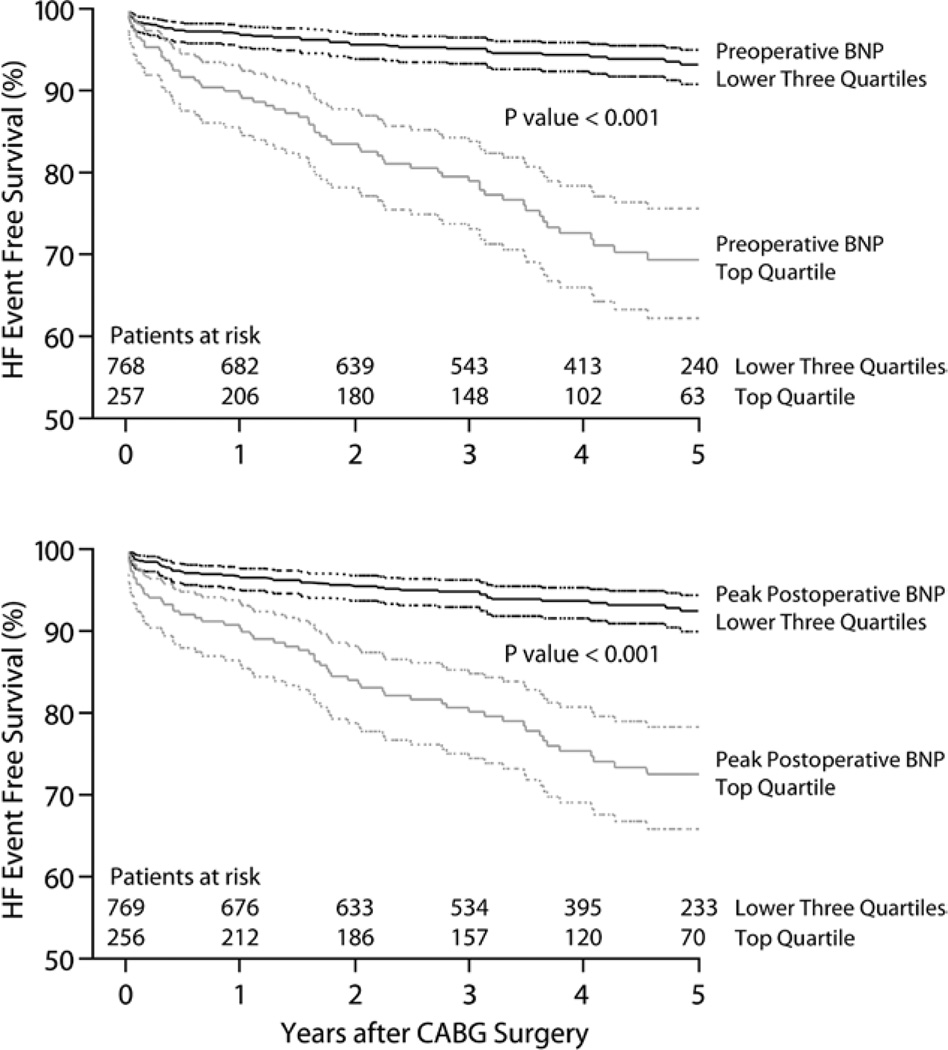
Results: One hundred five subjects experienced an HF event (median time to first event = 1.1 yr). Median follow-up for subjects who did not have an HF event = 4.2 yr. When individually added to the multivariable clinical model, higher preoperative and peak postoperative BNP concentrations each, independently associated with the HF outcome (log10 preoperative BNP hazard ratio = 1.93; 95% CI, 1.30-2.88; P = 0.001; log10 peak postoperative BNP hazard ratio = 3.38; 95% CI, 1.45-7.65; P = 0.003).
Conclusions: Increased perioperative BNP concentrations independently associate with HF hospitalization or HF death during the 5 yr after primary coronary artery bypass graft surgery. Clinical trials may be warranted to assess whether medical management focused on reducing preoperative and longitudinal postoperative BNP concentrations associates with decreased HF after coronary artery bypass graft surgery.
Figures
Similar articles
-
Plasma corin decreases after coronary artery bypass graft surgery and is associated with postoperative heart failure: a pilot study.J Cardiothorac Vasc Anesth. 2015 Apr;29(2):374-81. doi: 10.1053/j.jvca.2014.11.001. Epub 2014 Nov 11. J Cardiothorac Vasc Anesth. 2015. PMID: 25649697 Free PMC article.
-
Comparison of the utility of preoperative versus postoperative B-type natriuretic peptide for predicting hospital length of stay and mortality after primary coronary artery bypass grafting.Anesthesiology. 2010 Apr;112(4):842-51. doi: 10.1097/ALN.0b013e3181d23168. Anesthesiology. 2010. PMID: 20216395 Free PMC article.
-
Increased peak postoperative B-type natriuretic peptide predicts decreased longer-term physical function after primary coronary artery bypass graft surgery.Anesthesiology. 2011 Apr;114(4):807-16. doi: 10.1097/ALN.0b013e31820ef9c1. Anesthesiology. 2011. PMID: 21427536 Free PMC article.
-
Changes of natriuretic peptides predict hospital admissions in patients with chronic heart failure: a meta-analysis.JACC Heart Fail. 2014 Apr;2(2):148-58. doi: 10.1016/j.jchf.2013.11.007. JACC Heart Fail. 2014. PMID: 24720923 Review.
-
B-type natriuretic peptide-guided chronic heart failure therapy: a meta-analysis of 11 randomised controlled trials.Heart Lung Circ. 2013 Oct;22(10):852-60. doi: 10.1016/j.hlc.2013.03.077. Epub 2013 Apr 17. Heart Lung Circ. 2013. PMID: 23602555 Review.
Cited by
-
B-type natriuretic peptide as a surrogate marker for survival in patients undergoing cardiac surgery.J Thorac Dis. 2021 Feb;13(2):955-967. doi: 10.21037/jtd-20-2375. J Thorac Dis. 2021. PMID: 33717568 Free PMC article.
-
The Association Between Novel Biomarkers and 1-Year Readmission or Mortality After Cardiac Surgery.Ann Thorac Surg. 2018 Oct;106(4):1122-1128. doi: 10.1016/j.athoracsur.2018.04.084. Epub 2018 Jun 1. Ann Thorac Surg. 2018. PMID: 29864407 Free PMC article.
-
Pharmacogenomics of the Natriuretic Peptide System in Heart Failure.Curr Heart Fail Rep. 2017 Dec;14(6):536-542. doi: 10.1007/s11897-017-0365-5. Curr Heart Fail Rep. 2017. PMID: 29075957 Free PMC article. Review.
-
Six-month prognostic impact of hemodynamic profiling by short minimally invasive monitoring after cardiac surgery.J Cardiovasc Thorac Res. 2020;12(4):313-320. doi: 10.34172/jcvtr.2020.62. Epub 2020 Dec 13. J Cardiovasc Thorac Res. 2020. PMID: 33510881 Free PMC article.
-
Plasma corin decreases after coronary artery bypass graft surgery and is associated with postoperative heart failure: a pilot study.J Cardiothorac Vasc Anesth. 2015 Apr;29(2):374-81. doi: 10.1053/j.jvca.2014.11.001. Epub 2014 Nov 11. J Cardiothorac Vasc Anesth. 2015. PMID: 25649697 Free PMC article.
References
-
- Roger VL, Go AS, Lloyd-Jones DM, Adams RJ, Berry JD, Brown TM, Carnethon MR, Dai S, de Simone G, Ford ES, Fox CS, Fullerton HJ, Gillespie C, Greenlund KJ, Hailpern SM, Heit JA, Ho PM, Howard VJ, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Makuc DM, Marcus GM, Marelli A, Matchar DB, McDermott MM, Meigs JB, Moy CS, Mozaffarian D, Mussolino ME, Nichol G, Paynter NP, Rosamond WD, Sorlie PD, Stafford RS, Turan TN, Turner MB, Wong ND, Wylie-Rosett J. American Heart Association Statistics Committee and Stroke Statistics Subcommittee: Heart disease stroke statistics-2011 update A report from the American Heart Association. Circulation. 2011;123:e18. 09. - PMC - PubMed
-
- He J, Ogden LG, Bazzano LA, Vupputuri S, Loria C, Whelton PK. Risk factors for congestive heart failure in US men and women: NHANES I epidemiologic follow-up study. Arch Intern Med. 2001;161:996–202. - PubMed
-
- Fonarow GC, Abraham WT, Albert NM, Stough WG, Gheorghiade M, Greenberg BH, O’Connor CM, Pieper K, Sun JL, Yancy CW, Young JB. OPTIMIZE-HF Investigators and Hospitals: Factors identified as precipitating hospital admissions for heart failure and clinical outcomes Findings from OPTIMIZE-HF. Arch Intern Med. 2008;168:847–854. - PubMed
-
- Daniels LB, Maisel AS. Natriuretic peptides. J Am Coll Cardiol. 2007;50:2357–2368. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
