

Association between the MUC5B promoter polymorphism and survival in patients with idiopathic pulmonary fibrosis
- PMID: 23695349
- PMCID: PMC4545271
- DOI: 10.1001/jama.2013.5827
Association between the MUC5B promoter polymorphism and survival in patients with idiopathic pulmonary fibrosis
Abstract
Importance: Current prediction models of mortality in idiopathic pulmonary fibrosis (IPF), which are based on clinical and physiological parameters, have modest value in predicting which patients will progress. In addition to the potential for improving prognostic models, identifying genetic and molecular features that are associated with IPF mortality may provide insight into the underlying mechanisms of disease and inform clinical trials.
Objective: To determine whether the MUC5B promoter polymorphism (rs35705950), previously reported to be associated with the development of pulmonary fibrosis, is associated with survival in IPF.
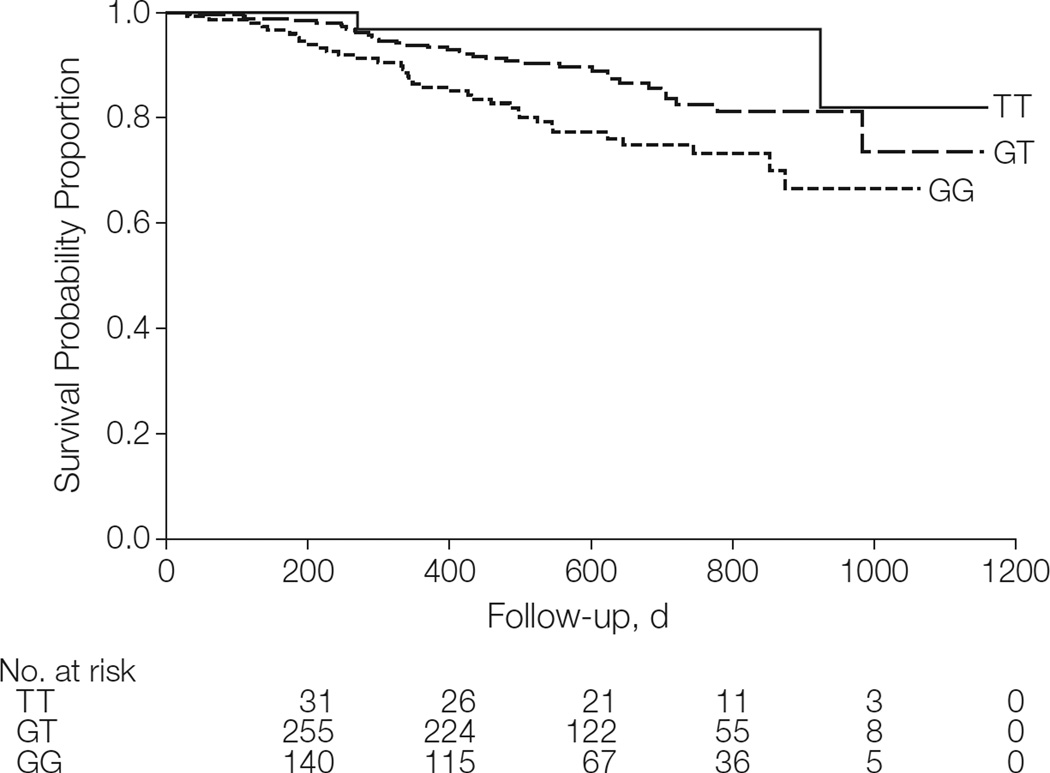
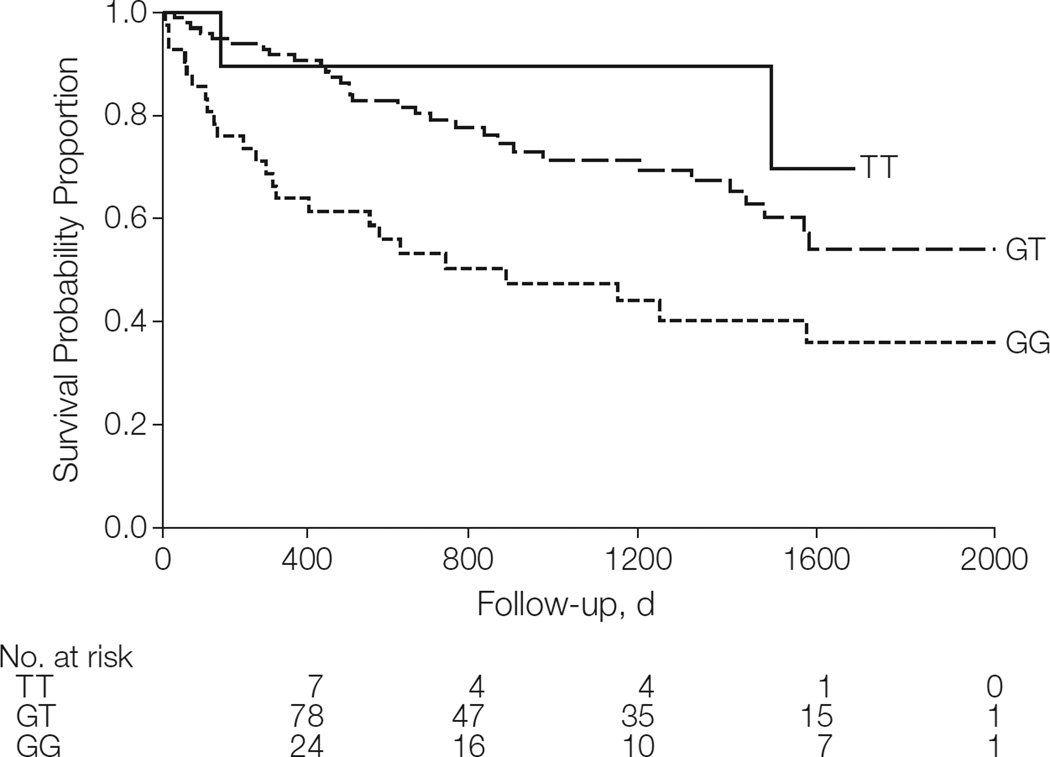
Design, setting, and participants: Retrospective study of survival in 2 independent cohorts of patients with IPF: the INSPIRE cohort, consisting of patients enrolled in the interferon-γ1b trial (n = 438; December 15, 2003-May 2, 2009; 81 centers in 7 European countries, the United States, and Canada), and the Chicago cohort, consisting of IPF participants recruited from the Interstitial Lung Disease Clinic at the University of Chicago (n = 148; 2007-2010). The INSPIRE cohort was used to model the association of the MUC5B genotype with survival, accounting for the effect of matrix metalloproteinase 7 (MMP-7) blood concentration and other demographic and clinical covariates. The Chicago cohort was used for replication of findings.
Main outcomes and measures: The primary end point was all-cause mortality.
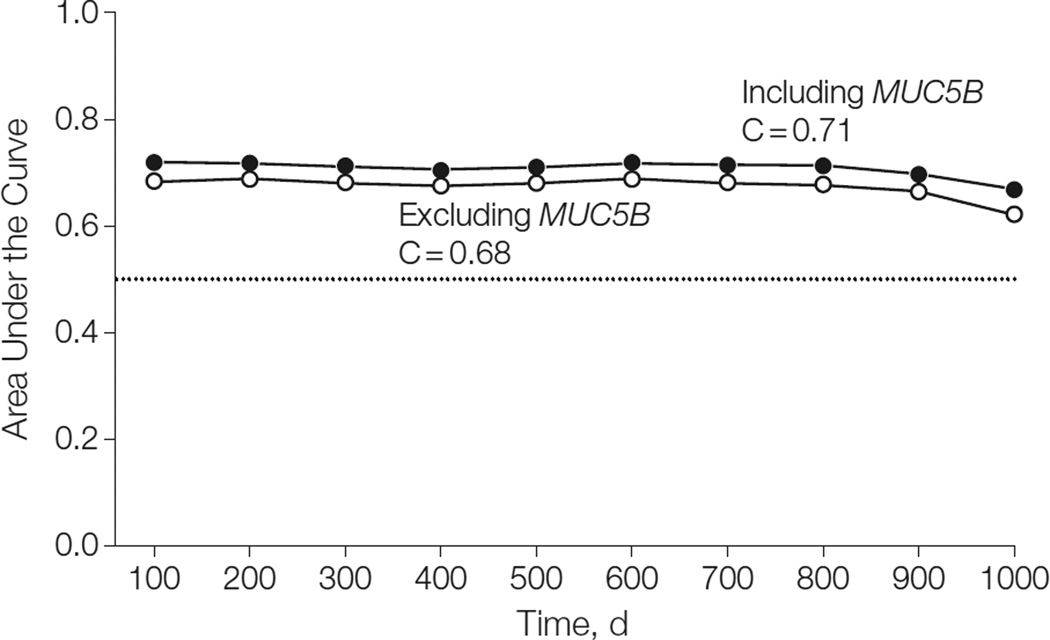
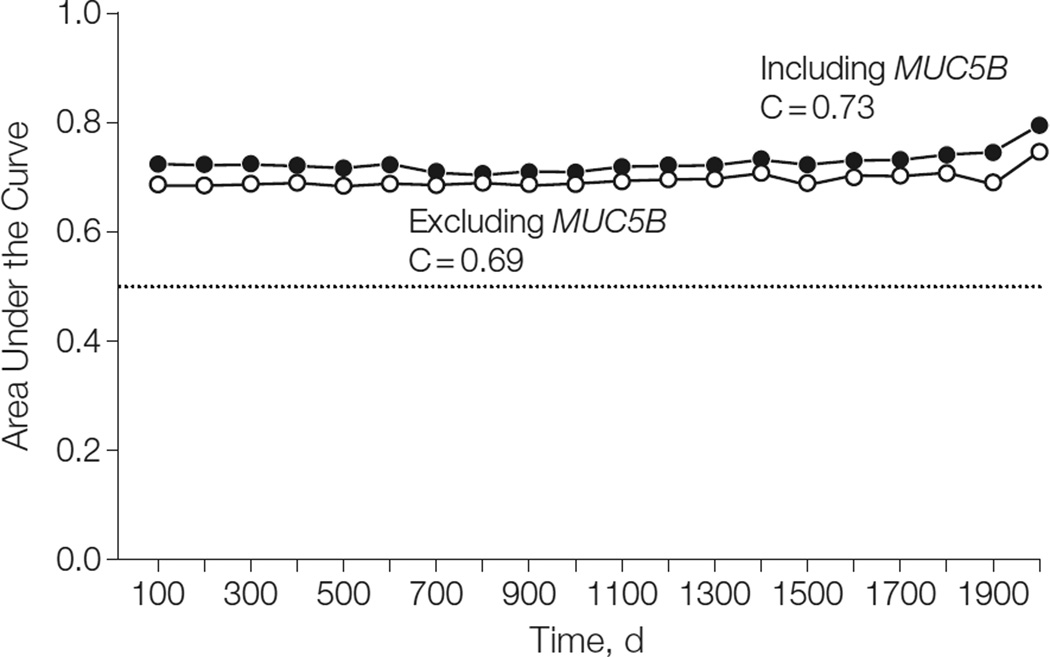
Results: The numbers of patients in the GG, GT, and TT genotype groups were 148 (34%), 259 (59%), and 31 (7%), respectively, in the INSPIRE cohort and 41 (28%), 98 (66%), and 9 (6%), respectively, in the Chicago cohort. The median follow-up period was 1.6 years for INSPIRE and 2.1 years for Chicago. During follow-up, there were 73 deaths (36 GG, 35 GT, and 2 TT) among INSPIRE patients and 64 deaths (26 GG, 36 GT, and 2 TT) among Chicago patients. The unadjusted 2-year cumulative incidence of death was lower among patients carrying 1 or more copies of the IPF risk allele (T) in both the INSPIRE cohort (0.25 [95% CI, 0.17-0.32] for GG, 0.17 [95% CI, 0.11-0.23] for GT, and 0.03 [95% CI, 0.00-0.09] for TT) and the Chicago cohort (0.50 [95% CI, 0.31-0.63] for GG, 0.22 [95% CI, 0.13-0.31] for GT, and 0.11 [95% CI, 0.00-0.28] for TT). In the INSPIRE cohort, the TT and GT genotypes (risk for IPF) were associated with improved survival compared with GG (hazard ratios, 0.23 [95% CI, 0.10-0.52] and 0.48 [95% CI, 0.31-0.72], respectively; P < .001). This finding was replicated in the Chicago cohort (hazard ratios, 0.15 [95% CI, 0.05-0.49] and 0.39 [95% CI, 0.21-0.70], respectively; P < .002). The observed association of MUC5B with survival was independent of age, sex, forced vital capacity, diffusing capacity of carbon monoxide, MMP-7, and treatment status. The addition of the MUC5B genotype to the survival models significantly improved the predictive accuracy of the model in both the INSPIRE cohort (C = 0.71 [95% CI, 0.64-0.75] vs C = 0.68 [95% CI, 0.61-0.73]; P < .001) and the Chicago cohort (C = 0.73 [95% CI, 0.62-0.78] vs C = 0.69 [95% CI, 0.59-0.75]; P = .01).
Conclusions and relevance: Among patients with IPF, a common risk polymorphism in MUC5B was significantly associated with improved survival. Further research is necessary to refine the risk estimates and to determine the clinical implications of these findings.
Conflict of interest statement
Figures
Comment in
-
YKL-40 in pediatric asthma, MUC5B promoter polymorphism in idiopathic pulmonary fibrosis, and esmolol in septic shock.Am J Respir Crit Care Med. 2014 May 1;189(9):1138-40. doi: 10.1164/rccm.201312-2253RR. Am J Respir Crit Care Med. 2014. PMID: 24787067 Free PMC article. No abstract available.
References
-
- Gross TJ, Hunninghake GW. Idiopathic pulmonary fibrosis. N Engl J Med. 2001;345(7):517–525. - PubMed
-
- Martinez FJ, Safrin S, Weycker D, et al. IPF Study Group. The clinical course of patients with idiopathic pulmonary fibrosis. Ann Intern Med. 2005;142(12 pt 1):963–967. - PubMed
-
- King TE, Jr, Tooze JA, Schwarz MI, Brown KR, Cherniack RM. Predicting survival in idiopathic pulmonary fibrosis: scoring system and survival model. Am J Respir Crit Care Med. 2001;164(7):1171–1181. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- F32 HL009961/HL/NHLBI NIH HHS/United States
- R01-HL095393/HL/NHLBI NIH HHS/United States
- R01 HL095397/HL/NHLBI NIH HHS/United States
- P01-HL092870/HL/NHLBI NIH HHS/United States
- RC2 HL101715/HL/NHLBI NIH HHS/United States
- P01 HL092870/HL/NHLBI NIH HHS/United States
- RC1-HL09961/HL/NHLBI NIH HHS/United States
- P50-HL0894932/HL/NHLBI NIH HHS/United States
- R01-HL095397/HL/NHLBI NIH HHS/United States
- R01-HL097163/HL/NHLBI NIH HHS/United States
- P50 HL084932/HL/NHLBI NIH HHS/United States
- R01 HL097163/HL/NHLBI NIH HHS/United States
- R01 HL095393/HL/NHLBI NIH HHS/United States
- RC2-HL101715/HL/NHLBI NIH HHS/United States
- RC1 HL099619/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
