

Prospective validation that vulnerable plaque associated with major adverse outcomes have larger plaque volume, less dense calcium, and more non-calcified plaque by quantitative, three-dimensional measurements using intravascular ultrasound with radiofrequency backscatter analysis : results from the ATLANTA I Study
- PMID: 23695823
- PMCID: PMC3790919
- DOI: 10.1007/s12265-013-9473-0
Prospective validation that vulnerable plaque associated with major adverse outcomes have larger plaque volume, less dense calcium, and more non-calcified plaque by quantitative, three-dimensional measurements using intravascular ultrasound with radiofrequency backscatter analysis : results from the ATLANTA I Study
Abstract
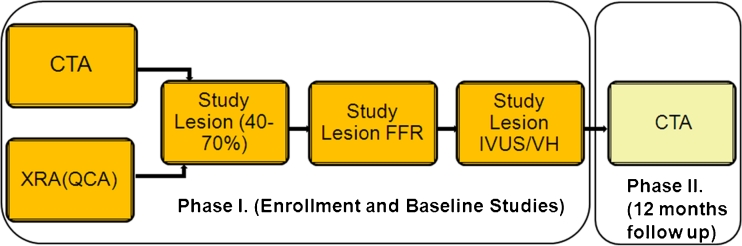
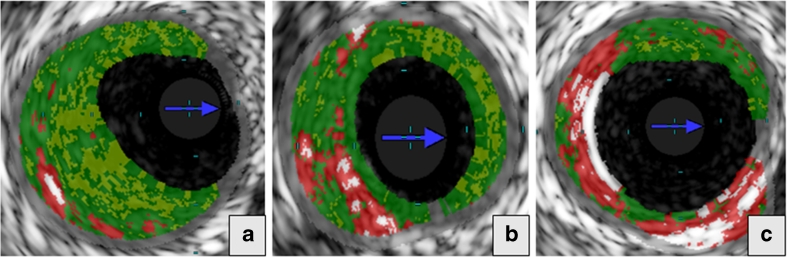
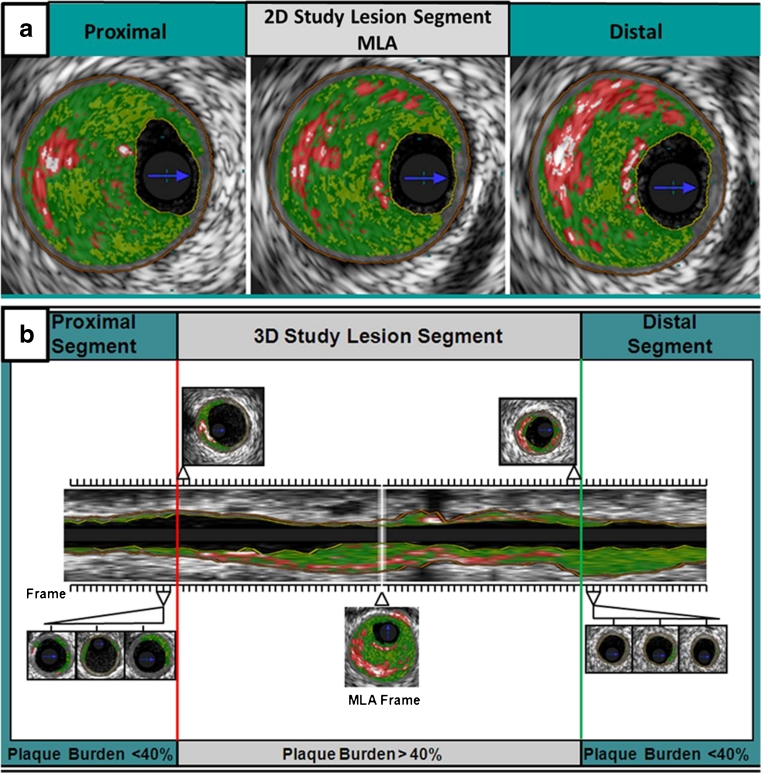
Whether quantitative, two-dimensional, and three-dimensional plaque measurements by intravascular ultrasound with radiofrequency backscatter (IVUS/VH) are different between intermediate lesions with or without major adverse cardiovascular events (MACE) is unknown. IVUS/VH-derived parameters were compared in 60 patients with an intermediate coronary lesion (40-70 %) between lesions that did or did not result in MACE over 12 months. IVUS/VH measurements were done at the site of the minimal lumen area (MLA) and on a per-plaque basis, defined by 40 % plaque burden. Pre-specified, adjudicated MACE events occurred in 5 of 60 patients (8.3 %). MACE lesions had larger plaque burden (65 % vs. 53 %, p = 0.004), less dense calcium (6.6 % vs. 14.7 %, p = 0.05), and more non-calcified plaque, mostly fibrofatty kind (17.6 % vs. 10 %, p = 0.02). Intermediate coronary lesions associated with MACE at 12 months have more plaque, less dense calcium, and more non-calcified plaque, particularly fibrofatty tissue by IVUS/VH.
Trial registration: ClinicalTrials.gov NCT00817102.
Figures



References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
