

Clinical use of colistin induces cross-resistance to host antimicrobials in Acinetobacter baumannii
- PMID: 23695834
- PMCID: PMC3663567
- DOI: 10.1128/mBio.00021-13
Clinical use of colistin induces cross-resistance to host antimicrobials in Acinetobacter baumannii
Abstract
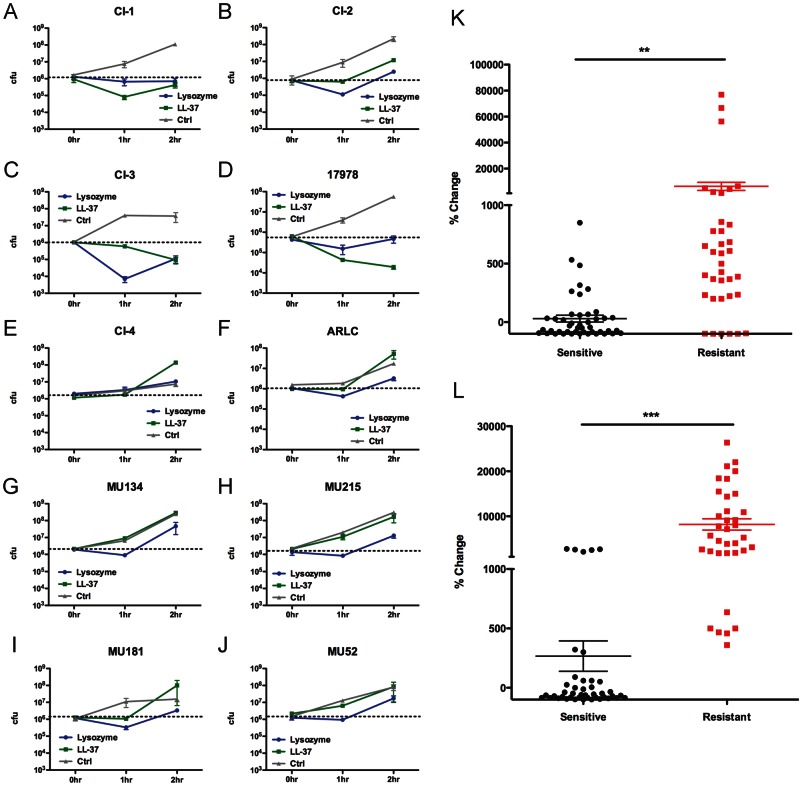
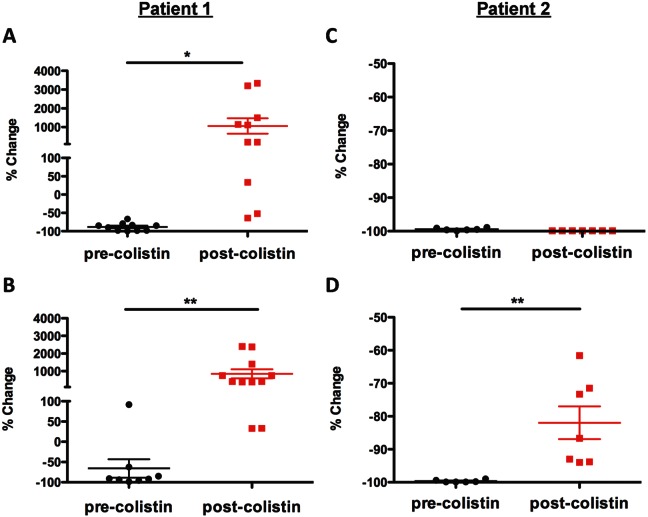
The alarming rise in antibiotic resistance has led to an increase in patient mortality and health care costs. This problem is compounded by the absence of new antibiotics close to regulatory approval. Acinetobacter baumannii is a human pathogen that causes infections primarily in patients in intensive care units (ICUs) and is highly antibiotic resistant. Colistin is one of the last-line antibiotics for treating A. baumannii infections; however, colistin-resistant strains are becoming increasingly common. This cationic antibiotic attacks negatively charged bacterial membranes in a manner similar to that seen with cationic antimicrobials of the innate immune system. We therefore set out to determine if the increasing use of colistin, and emergence of colistin-resistant strains, is concomitant with the generation of cross-resistance to host cationic antimicrobials. We found that there is indeed a positive correlation between resistance to colistin and resistance to the host antimicrobials LL-37 and lysozyme among clinical isolates. Importantly, isolates obtained before and after treatment of individual patients demonstrated that colistin use correlated with increased resistance to cationic host antimicrobials. These data reveal the overlooked risk of inducing cross-resistance to host antimicrobials when treating patients with colistin as a last-line antibiotic. IMPORTANCE Increased use of the cationic antibiotic colistin to treat multidrug-resistant Acinetobacter baumannii has led to the development of colistin-resistant strains. Here we report that treatment of patients with colistin can induce not only increased resistance to colistin but also resistance to host cationic antimicrobials. This worrisome finding likely represents an example of a broader trend observed in other bacteria against which colistin is used therapeutically such as Pseudomonas aeruginosa and Klebsiella pneumoniae. Furthermore, these data suggest that the possible future use of an array of cationic antimicrobial peptides in development as therapeutics may have unintended negative consequences, eventually leading to the generation of hypervirulent strains that are resistant to innate host defenses. The potential for the induction of cross-resistance to innate immune antimicrobials should be considered during the development of new therapeutics.
Figures
References
-
- de Kraker ME, Wolkewitz M, Davey PG, Koller W, Berger J, Nagler J, Icket C, Kalenic S, Horvatic J, Seifert H, Kaasch AJ, Paniara O, Argyropoulou A, Bompola M, Smyth E, Skally M, Raglio A, Dumpis U, Kelmere AM, Borg M, Xuereb D, Ghita MC, Noble M, Kolman J, Grabljevec S, Turner D, Lansbury L, Grundmann H. 2011. Clinical impact of antimicrobial resistance in European hospitals: excess mortality and length of hospital stay related to methicillin-resistant Staphylococcus aureus bloodstream infections. Antimicrob. Agents Chemother. 55:1598–1605 - PMC - PubMed
-
- Maragakis LL, Perencevich EN, Cosgrove SE. 2008. Clinical and economic burden of antimicrobial resistance. Expert Rev. Anti Infect. Ther. 6:751–763 - PubMed
-
- Salgado CD, O’Grady N, Farr BM. 2005. Prevention and control of antimicrobial-resistant infections in intensive care patients. Crit. Care Med. 33:2373–2382 - PubMed
-
- Vandijck DM, Depaemelaere M, Labeau SO, Depuydt PO, Annemans L, Buyle FM, Oeyen S, Colpaert KE, Peleman RP, Blot SI, Decruyenaere JM. 2008. Daily cost of antimicrobial therapy in patients with intensive care unit-acquired, laboratory-confirmed bloodstream infection. Int. J. Antimicrob. Agents 31:161–165 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
