

Depth of invasion, tumor budding, and worst pattern of invasion: prognostic indicators in early-stage oral tongue cancer
- PMID: 23696499
- PMCID: PMC4229066
- DOI: 10.1002/hed.23380
Depth of invasion, tumor budding, and worst pattern of invasion: prognostic indicators in early-stage oral tongue cancer
Abstract
Background: Oral (mobile) tongue squamous cell carcinoma (SCC) is characterized by a highly variable prognosis in early-stage disease (T1/T2 N0M0). The ability to classify early oral tongue SCCs into low-risk and high-risk categories would represent a major advancement in their management.
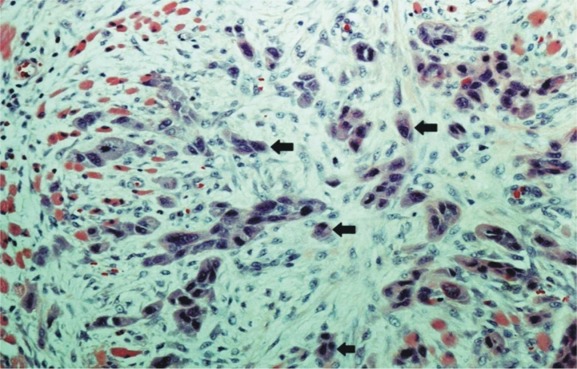
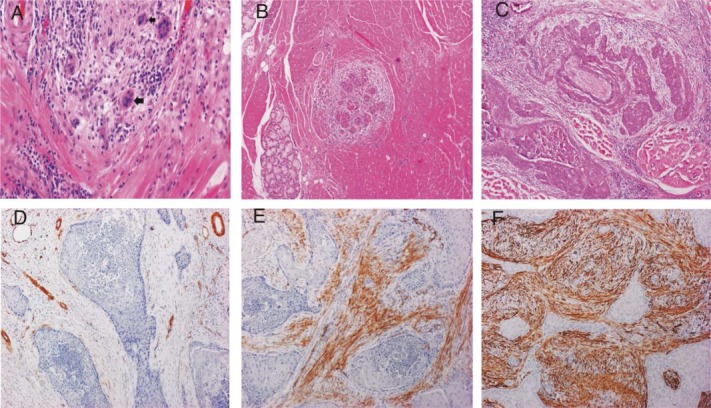
Methods: Depth of invasion, tumor budding, histologic risk-assessment score (HRS), and cancer-associated fibroblast (CAF) density were studied in 233 cases of T1/T2 N0M0 oral tongue SCC managed in 5 university hospitals in Finland.
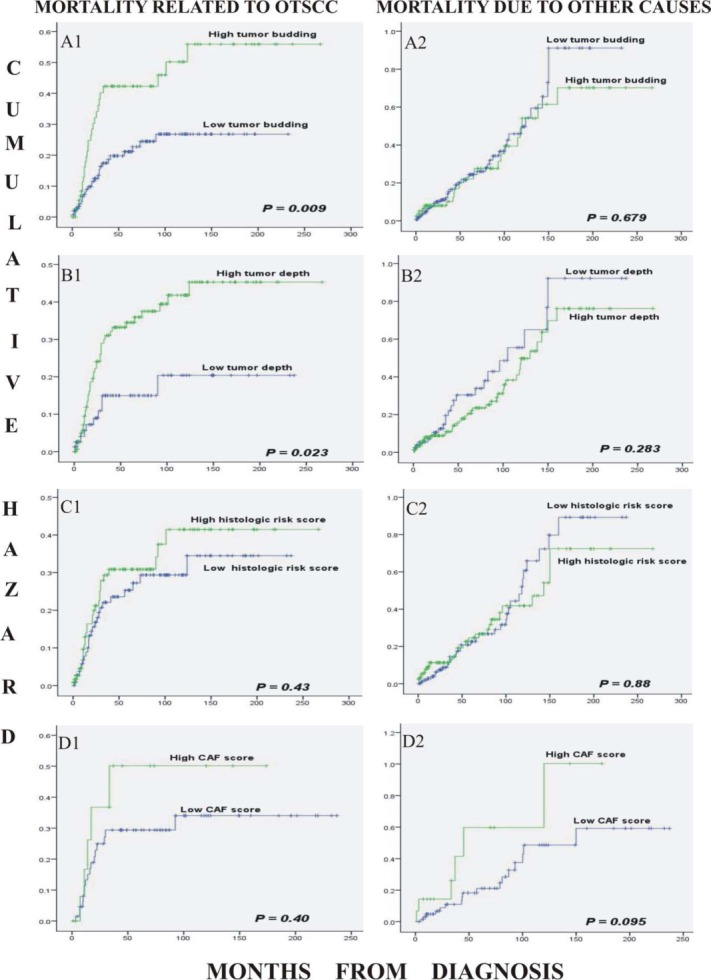
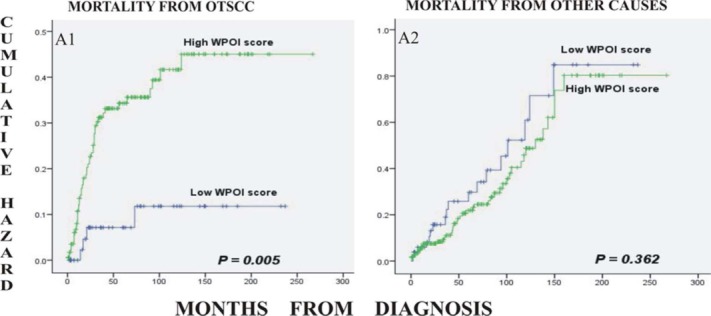
Results: Tumor budding (≥5 clusters at the invasive front of the tumor) and depth of invasion (≥4 mm) were associated with poor prognosis in patients with early oral tongue SCC (hazard ratio [HR], 2.04; 95% confidence interval [CI], 1.17-3.55; HR, 2.55; 95% CI, 1.25-5.20, respectively) after multivariate analysis. The HRS and CAF density did not predict survival. However, high-risk worst pattern of invasion (WPOI), a component of HRS, was also an independent prognostic factor (HR, 4.47; 95% CI, 1.59-12.51).
Conclusion: Analyzing the depth of invasion, tumor budding, and/or WPOI in prognostication and treatment planning of T1/T2 N0M0 oral tongue SCC is recommended.
Keywords: cancer-associated fibroblast; depth of invasion; disease-specific mortality; histologic risk score; oral tongue squamous cell carcinoma; prognosis; tumor budding; worst pattern of invasion.
© 2013 The Authors. Head & Neck published by Wiley Periodicals, Inc.
Figures
References
-
- Ganly I, Patel S, Shah J. Early stage squamous cell cancer of the oral tongue—clinicopathologic features affecting outcome. Cancer. 2012;118:101–111. - PubMed
-
- Ho CM, Lam KH, Wei WI, Lau SK, Lam LK. Occult lymph node metastasis in small oral tongue cancers. Head Neck. 1992;14:359–363. - PubMed
-
- Kellermann MG, Sobral LM, da Silva SD, et al. Myofibroblasts in the stroma of oral squamous cell carcinoma are associated with poor prognosis. Histopathology. 2007;51:849–853. - PubMed
-
- Keski–Säntti H, Atula T, Tikka J, Hollmén J, Mäkitie AA, Leivo I. Predictive value of histopathologic parameters in early squamous cell carcinoma of oral tongue. Oral Oncol. 2007;43:1007–1013. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
