

Development and evaluation of a genetic risk score for obesity
- PMID: 23701538
- PMCID: PMC3671353
- DOI: 10.1080/19485565.2013.774628
Development and evaluation of a genetic risk score for obesity
Abstract
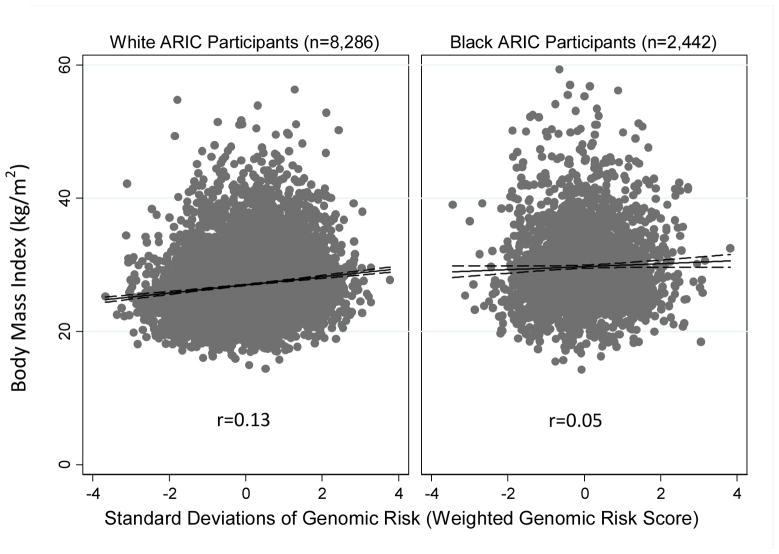
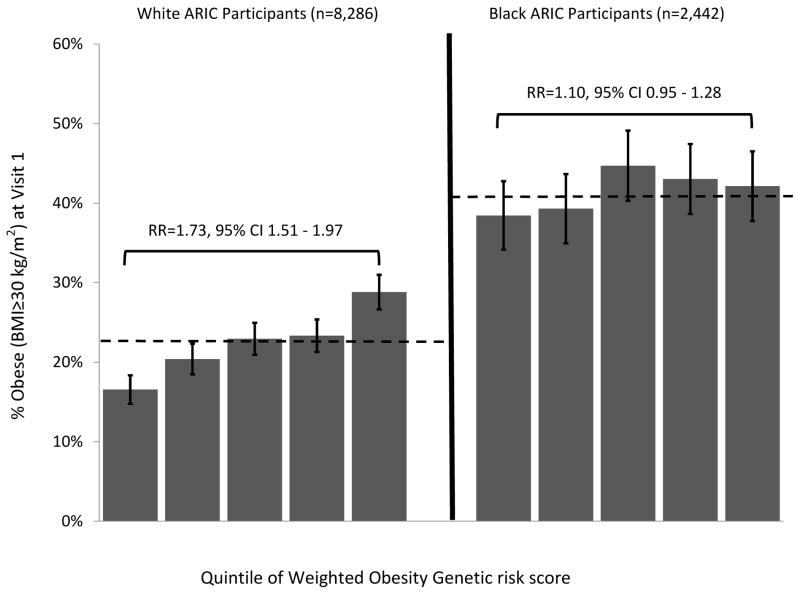
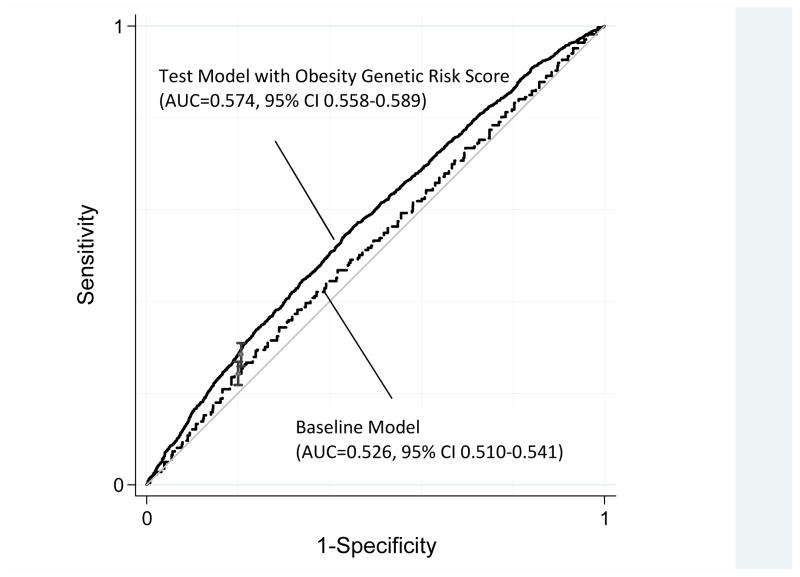
Multi-locus profiles of genetic risk, so-called "genetic risk scores," can be used to translate discoveries from genome-wide association studies into tools for population health research. We developed a genetic risk score for obesity from results of 16 published genome-wide association studies of obesity phenotypes in European-descent samples. We then evaluated this genetic risk score using data from the Atherosclerosis Risk in Communities (ARIC) cohort GWAS sample (N = 10,745, 55% female, 77% white, 23% African American). Our 32-locus GRS was a statistically significant predictor of body mass index (BMI) and obesity among ARIC whites [for BMI, r = 0.13, p<1 × 10(-30); for obesity, area under the receiver operating characteristic curve (AUC) = 0.57 (95% CI 0.55-0.58)]. The GRS predicted differences in obesity risk net of demographic, geographic, and socioeconomic information. The GRS performed less well among African Americans. The genetic risk score we derived from GWAS provides a molecular measurement of genetic predisposition to elevated BMI and obesity.[Supplemental materials are available for this article. Go to the publisher's online edition of Biodemography and Social Biology for the following resource: Supplement to Development & Evaluation of a Genetic Risk Score for Obesity.].
Figures
References
Publication types
MeSH terms
Grants and funding
- R01 HL059367/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- U01 HG004402/HG/NHGRI NIH HHS/United States
- R36 HS020524/HS/AHRQ HHS/United States
- T32 HD007376/HD/NICHD NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- R01 HL087641/HL/NHLBI NIH HHS/United States
- R01 AG032282/AG/NIA NIH HHS/United States
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- UL1RR025005/RR/NCRR NIH HHS/United States
- T32-AG000029/AG/NIA NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- AG032282/AG/NIA NIH HHS/United States
- G0601483/MRC_/Medical Research Council/United Kingdom
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- R01 HL086694/HL/NHLBI NIH HHS/United States
- R01 MH077874/MH/NIMH NIH HHS/United States
- 1R36HS020524-01/HS/AHRQ HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- G0100527/MRC_/Medical Research Council/United Kingdom
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical