

Review
doi: 10.1016/j.ccm.2013.02.005.
Epub 2013 Apr 15.
Evaluation of respiratory disease
Affiliations
- PMID: 23702170
- PMCID: PMC3751804
- DOI: 10.1016/j.ccm.2013.02.005
Item in Clipboard
Review
Evaluation of respiratory disease
Clin Chest Med.
2013 Jun.
Abstract
The spectrum of HIV-associated pulmonary diseases is broad. Opportunistic infections, neoplasms, and noninfectious complications are all major considerations. Clinicians caring for persons infected with HIV must have a systematic approach. The approach begins with a thorough history and physical examination and often involves selected laboratory tests and a chest radiograph. Frequently, the clinical, laboratory, and chest radiographic presentation suggests a specific diagnosis or a few diagnoses, which then prompts specific diagnostic testing and treatment. This article presents an overview of the evaluation of respiratory disease in persons with HIV/AIDS.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures
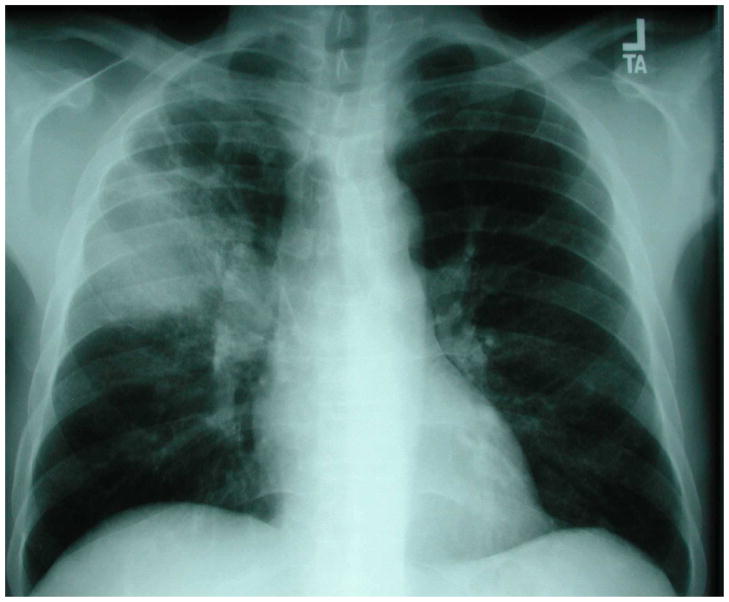
Chest radiograph of an HIV-infected person with multilobar consolidation due to Streptococcus pneumoniae detected in two blood cultures. Chest radiograph courtesy of Laurence Huang, MD.
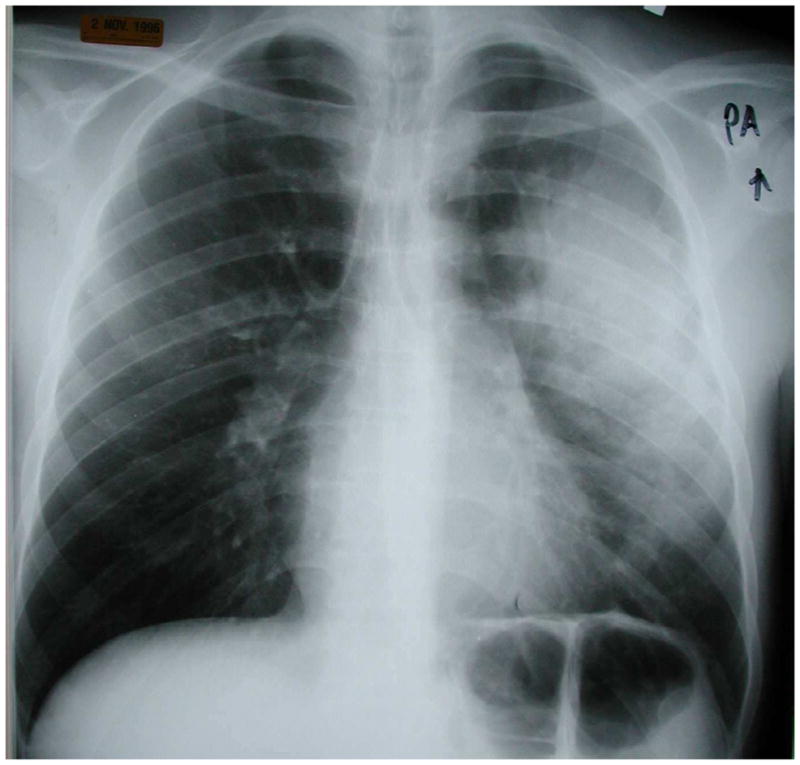
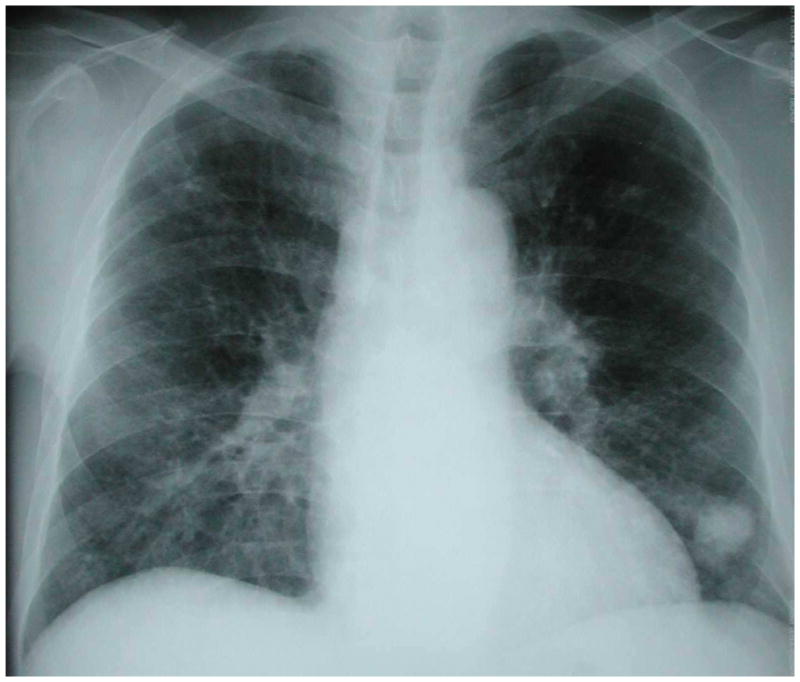
Chest radiograph of an HIV-infected person, CD4 cell count greater than 200 cells/μL, revealing right upper lobe consolidation with areas of cavitation. Sputum acid-fast bacillus stain was positive and sputum cultures grew Mycobacterium tuberculosis. Chest radiograph courtesy of Laurence Huang, MD.
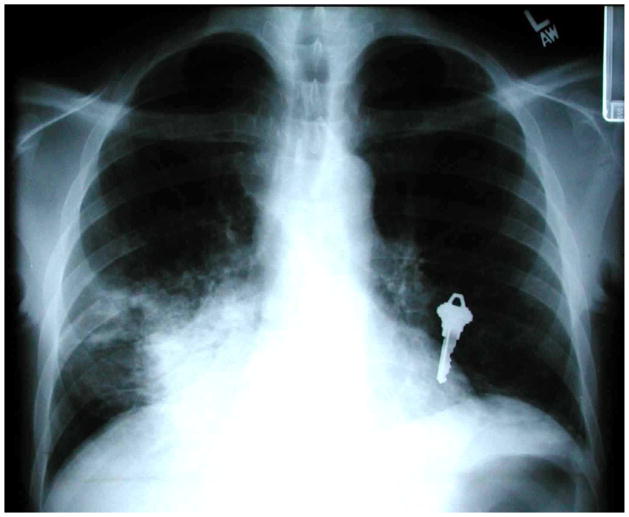
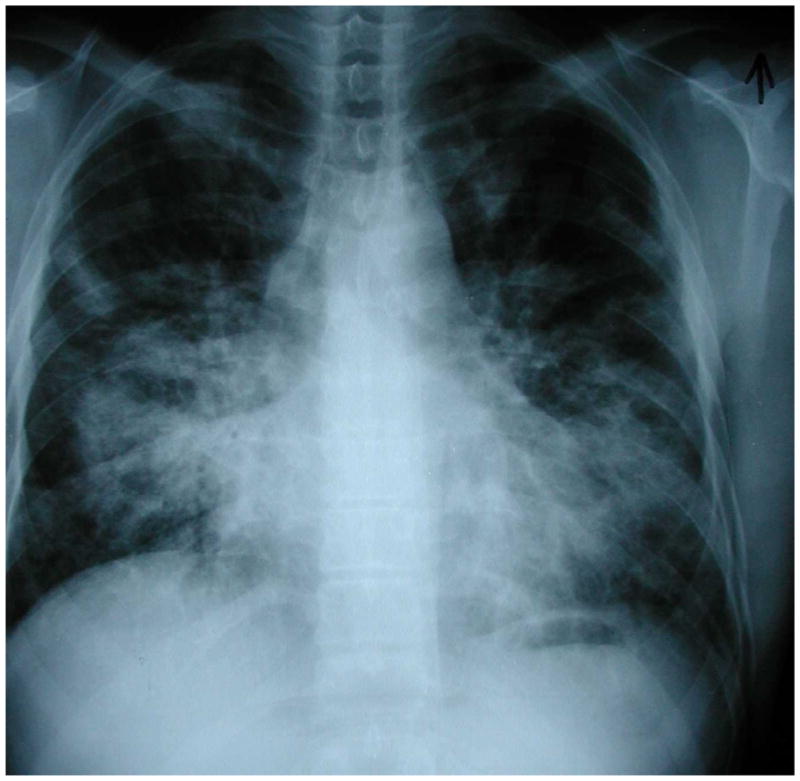
Chest radiograph of an HIV-infected person, CD4 cell count less than 200 cells/μL, revealing right lower lung consolidation. Sputum acid-fast bacillus stains were negative but sputum cultures grew Mycobacterium tuberculosis that was mono-rifampin-resistant. In this case, the key to the diagnosis of tuberculosis was knowledge of the patient’s CD4 cell count and an understanding that tuberculosis can present with this pattern in HIV-infected individuals with advanced immunosuppression. Chest radiograph courtesy of Laurence Huang, MD.
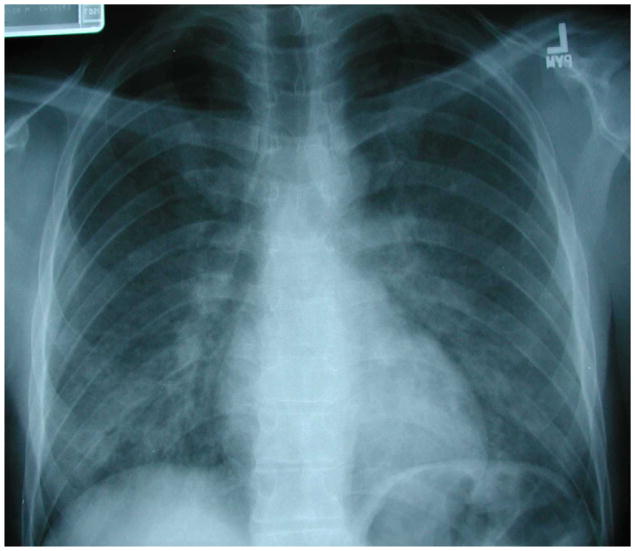
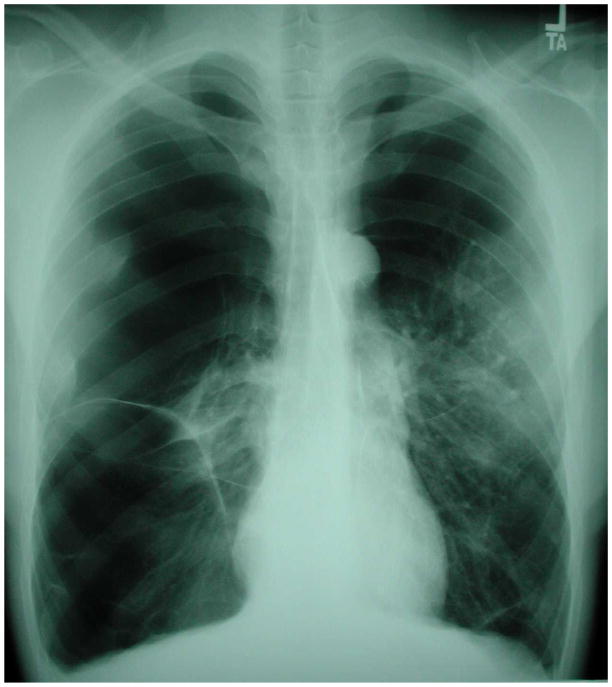
Chest radiograph of an HIV-infected person, CD4 cell count less than 200 cells/μL, with bilateral, symmetric granular opacities due to Pneumocystis pneumonia. Microscopic examination of bronchoscopy with bronchoalveolar lavage (BAL) fluid demonstrated characteristic Pneumocystis cystic and trophic forms. Chest radiograph courtesy of Laurence Huang, MD.
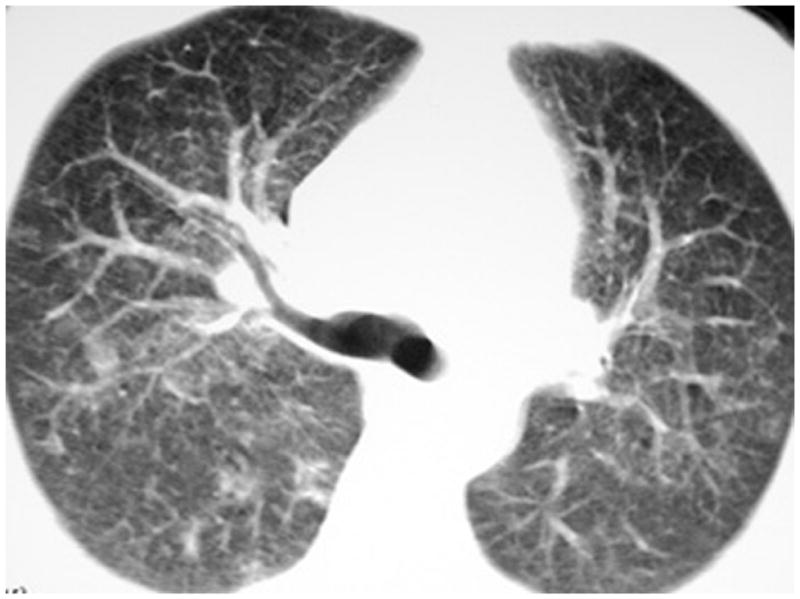
Chest high resolution computed tomographic (HRCT) scan of an HIV-infected person, CD4 cell count less than 200 cells/μL, with patchy ground-glass opacities due to Pneumocystis pneumonia. Microscopic examination of induced sputum demonstrated characteristic Pneumocystis cystic and trophic forms. This individual’s chest radiograph one day prior to chest HRCT was normal, demonstrating the increased sensitivity of chest HRCT compared to chest radiography for Pneumocystis pneumonia. Chest HRCT scan courtesy of Laurence Huang, MD.
Chest radiograph of an HIV-infected person, CD4 cell count less than 200 cells/μL, with left lower lobe lung mass that was initially concerning for lung cancer. CT-guided fine needle aspiration revealed Cryptococcus neoformans. Chest radiograph courtesy of Laurence Huang, MD.
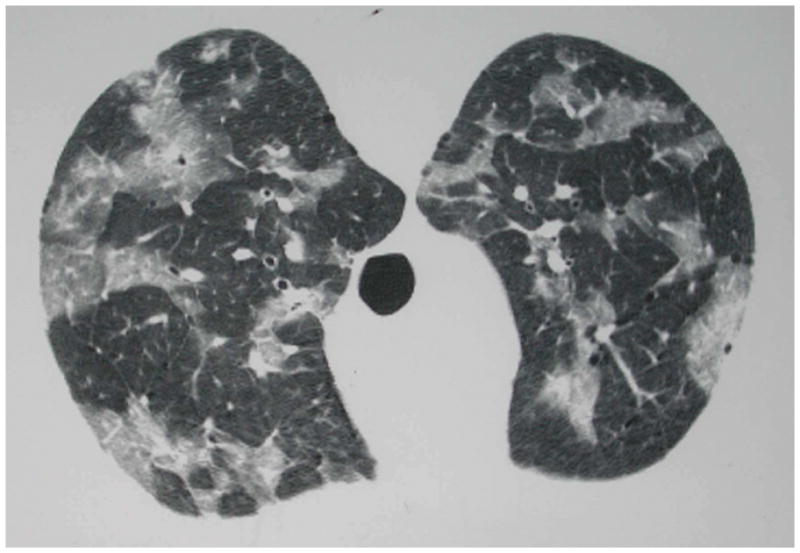
Chest high resolution computed tomographic (HRCT) scan of an HIV-infected person, CD4 cell count less than 50 cells/μL, with patchy ground-glass opacities due to Cytomegalovirus (CMV). The patient was initially thought to have Pneumocystis pneumonia but bronchoscopy with bronchoalveolar lavage was negative for Pneumocystis cystic and trophic forms. The patient then underwent video-assisted thoracoscopic surgical biopsy which established the diagnosis of CMV. Chest HRCT scan courtesy of Laurence Huang, MD.

Characteristic violaceous Kaposi sarcoma lesions seen in the trachea of an HIV-infected person, CD4 cell count less than 100 cells/μL. Image courtesy of Laurence Huang, MD.
Chest radiograph of an HIV-infected person, CD4 cell count less than 100 cells/μL, demonstrating the characteristic bilateral, middle and lower lung zone, perihilar or central distribution of abnormalities of pulmonary Kaposi sarcoma. This individual had no evidence of mucocutaneous Kaposi sarcoma and the diagnosis of pulmonary Kaposi sarcoma was established by bronchoscopy with visualization of multiple, characteristic Kaposi sarcoma lesions (see Figure 7). Chest radiograph courtesy of Laurence Huang, MD.
Chest radiograph of an HIV-infected person with hyperinflation, flattened diaphragms, increased radiolucency of the lungs, and multiple, large bullae from severe COPD. Chest radiograph courtesy of Laurence Huang, MD.
Similar articles
-
Respiratory complications in Brazilian patients infected with human immunodeficiency virus.Rev Inst Med Trop Sao Paulo. 1993 Mar-Apr;35(2):129-39. doi: 10.1590/s0036-46651993000200004. Rev Inst Med Trop Sao Paulo. 1993. PMID: 8284597
-
Respiratory emergencies in HIV-infected persons.Emerg Med Clin North Am. 2010 May;28(2):283-98, Table of Contents. doi: 10.1016/j.emc.2010.01.014. Emerg Med Clin North Am. 2010. PMID: 20413012
-
[Pulmonary manifestations in HIV-infected patients: a diagnostic approach].Rev Mal Respir. 2014 Dec;31(10):903-15. doi: 10.1016/j.rmr.2014.04.106. Epub 2014 Aug 31. Rev Mal Respir. 2014. PMID: 25496788 Review. French.
-
Chest X-ray evaluation of pneumonia-like syndromes in smear negative HIV-positive patients with atypical chest x-ray. Findings in Ethiopian setting.Ethiop Med J. 2011 Jan;49(1):35-42. Ethiop Med J. 2011. PMID: 21456470
-
HIV-associated bacterial pneumonia.Clin Chest Med. 2013 Jun;34(2):205-16. doi: 10.1016/j.ccm.2013.01.006. Epub 2013 Apr 8. Clin Chest Med. 2013. PMID: 23702171 Review.
Cited by
-
Epidemic and pandemic viral infections: impact on tuberculosis and the lung: A consensus by the World Association for Infectious Diseases and Immunological Disorders (WAidid), Global Tuberculosis Network (GTN), and members of the European Society of Clinical Microbiology and Infectious Diseases Study Group for Mycobacterial Infections (ESGMYC).Eur Respir J. 2020 Oct 1;56(4):2001727. doi: 10.1183/13993003.01727-2020. Print 2020 Oct. Eur Respir J. 2020. PMID: 32586885 Free PMC article. Review.
-
Toxoplasmosis complicating lung cancer: a case report.Int Med Case Rep J. 2015 Jan 22;8:37-40. doi: 10.2147/IMCRJ.S76488. eCollection 2015. Int Med Case Rep J. 2015. PMID: 25653562 Free PMC article.
-
Pulmonary cryptococcosis presenting as acute severe respiratory distress in a newly diagnosed HIV patient in Tanzania: a case report.Clin Case Rep. 2015 Sep;3(9):749-52. doi: 10.1002/ccr3.337. Epub 2015 Aug 11. Clin Case Rep. 2015. PMID: 26401280 Free PMC article.
-
Diagnostic discrepancy between bronchoalveolar lavage and transbronchial biopsy from bronchoscopies of HIV patients with pneumonia: toward an integral diagnosis.HIV AIDS (Auckl). 2018 Jul 6;10:115-123. doi: 10.2147/HIV.S161899. eCollection 2018. HIV AIDS (Auckl). 2018. PMID: 30013402 Free PMC article.
-
Recent Insights into the HIV/AIDS Pandemic.Microb Cell. 2016 Sep 5;3(9):451-475. doi: 10.15698/mic2016.09.529. Microb Cell. 2016. PMID: 28357381 Free PMC article. Review.
References
-
- Huang L, Stansell JD. AIDS and the lung. Med Clin North Am. 1996;80:775–801. - PubMed
-
- Kovacs JA, Hiemenz JW, Macher AM, et al. Pneumocystis carinii pneumonia: a comparison between patients with the acquired immunodeficiency syndrome and patients with other immunodeficiencies. Ann Intern Med. 1984;100:663–671. - PubMed
-
- Chaisson RE, Schecter GF, Theuer CP, et al. Tuberculosis in patients with the acquired immunodeficiency syndrome. Clinical features, response to therapy, and survival. Am Rev Respir Dis. 1987;136:570–574. - PubMed
-
- Jacob JT, Mehta AK, Leonard MK. Acute forms of tuberculosis in adults. Am J Med. 2009;122:12–17. - PubMed
-
- Chuck SL, Sande MA. Infections with Cryptococcus neoformans in the acquired immunodeficiency syndrome. N Engl J Med. 1989;321:794–799. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
