

Clinical outcomes strongly associated with the degree of reperfusion achieved in target mismatch patients: pooled data from the Diffusion and Perfusion Imaging Evaluation for Understanding Stroke Evolution studies
- PMID: 23704106
- PMCID: PMC3810454
- DOI: 10.1161/STROKEAHA.111.000371
Clinical outcomes strongly associated with the degree of reperfusion achieved in target mismatch patients: pooled data from the Diffusion and Perfusion Imaging Evaluation for Understanding Stroke Evolution studies
Abstract
Background and purpose: To investigate relationships between the degree of early reperfusion achieved on perfusion-weighted imaging and clinical outcomes in the Diffusion and Perfusion Imaging Evaluation for Understanding Stroke Evolution studies. We hypothesized that there would be a strong correlation between the degree of reperfusion achieved and clinical outcomes in target mismatch (TMM) patients.
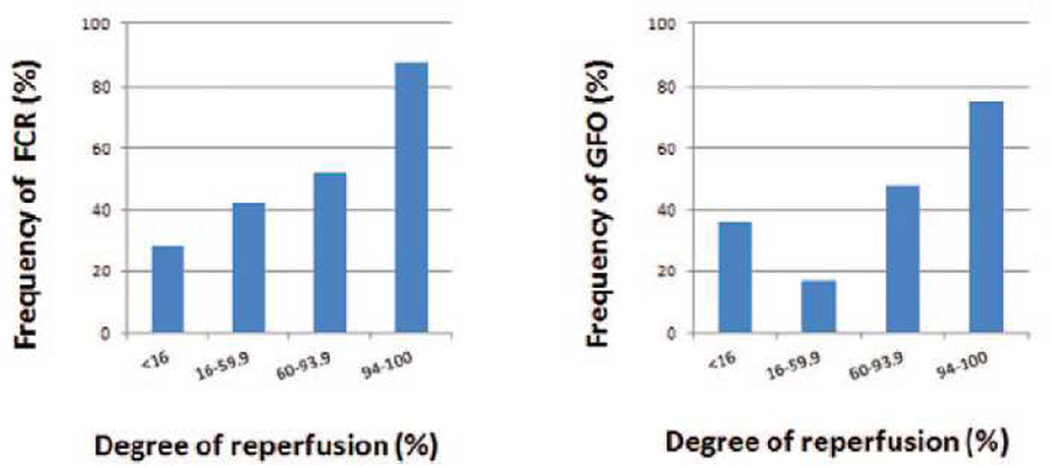
Methods: The degree of reperfusion was calculated on the basis of the difference in perfusion-weighted imaging volumes (time to maximum of tissue residue function [Tmax]>6 s) between the baseline MRI and the early post-treatment follow-up scan. Patients were grouped into quartiles, on the basis of degree of reperfusion achieved, and the association between the degree of reperfusion and clinical outcomes in TMM and no TMM patients was assessed. Favorable clinical response was determined at day 30 on the basis of the National Institutes of Health Stroke Scale and good functional outcome was defined as a modified Rankin Scale score ≤2 at day 90.
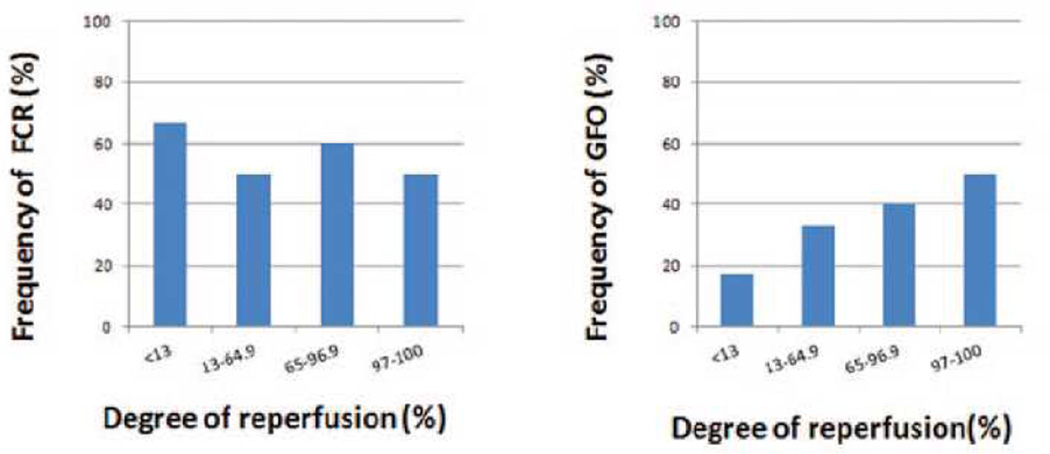
Results: This study included 121 patients; 98 of these had TMM. The median degree of reperfusion achieved was not different in TMM patients (60%) versus No TMM patients (64%; P=0.604). The degree of reperfusion was strongly correlated with both favorable clinical response (P<0.001) and good functional outcome (P=0.001) in TMM patients; no correlation was present in no TMM. The frequency of achieving favorable clinical response or good functional outcome was significantly higher in TMM patients in the highest reperfusion quartile versus the lower 3 quartiles (88% versus 41% as odds ratio, 10.3; 95% confidence interval, 2.8-37.5; and 75% versus 34% as odds ratio, 5.9; 95% confidence interval, 2.1-16.7, respectively). A receiver operating characteristic curve analysis identified 90% as the optimal reperfusion threshold for predicting good functional outcomes.
Conclusion: The degree of reperfusion documented on perfusion-weighted imaging after reperfusion therapies corresponds closely with clinical outcomes in TMM patients. Reperfusion of ≥90% of the perfusion lesion is an appropriate goal for reperfusion therapies to aspire to.
Keywords: acute stroke; endovascular treatment; magnetic resonance imaging; perfusion-weighted imaging; reperfusion.
Figures
References
-
- Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: A meta-analysis. Stroke. 2007;38:967–973. - PubMed
-
- Saver JL, Jahan R, Levy EI, Jovin TG, Baxter B, Nogueira RG, et al. Solitaire flow restoration device versus the merci retriever in patients with acute ischaemic stroke (SWIFT): A randomised, parallel-group, non-inferiority trial. Lancet. 2012;380:1241–1249. - PubMed
-
- Davis SM, Donnan GA, Parsons MW, Levi C, Butcher KS, Peeters A, et al. Effects of alteplase beyond 3 h after stroke in the echoplanar imaging thrombolytic evaluation trial (EPITHET): A placebo-controlled randomised trial. Lancet Neurol. 2008;7:299–309. - PubMed
-
- Parsons M, Spratt N, Bivard A, Campbell B, Chung K, Miteff F, et al. A randomized trial of tenecteplase versus alteplase for acute ischemic stroke. N Engl J Med. 2012;366:1099–1107. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
