

Risk profiles and antithrombotic treatment of patients newly diagnosed with atrial fibrillation at risk of stroke: perspectives from the international, observational, prospective GARFIELD registry
- PMID: 23704912
- PMCID: PMC3660389
- DOI: 10.1371/journal.pone.0063479
Risk profiles and antithrombotic treatment of patients newly diagnosed with atrial fibrillation at risk of stroke: perspectives from the international, observational, prospective GARFIELD registry
Abstract
Background: Limited data are available on the characteristics, clinical management, and outcomes of patients with atrial fibrillation at risk of stroke, from a worldwide perspective. The aim of this study was to describe the baseline characteristics and initial therapeutic management of patients with non-valvular atrial fibrillation across the spectrum of sites at which these patients are treated.
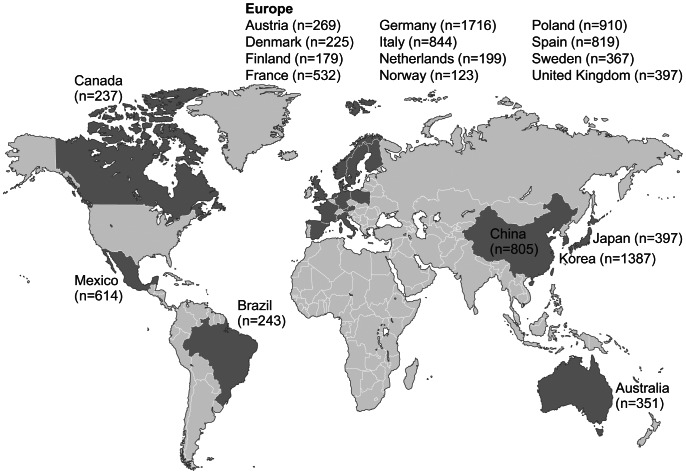
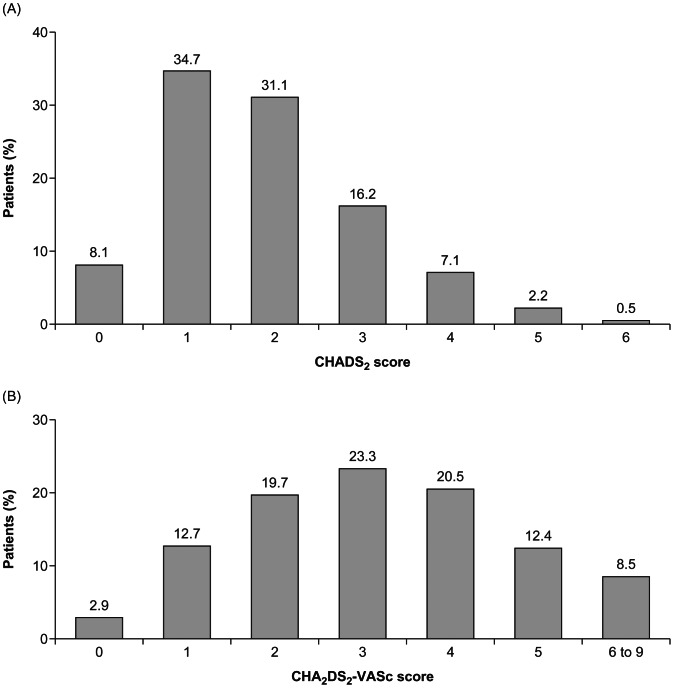
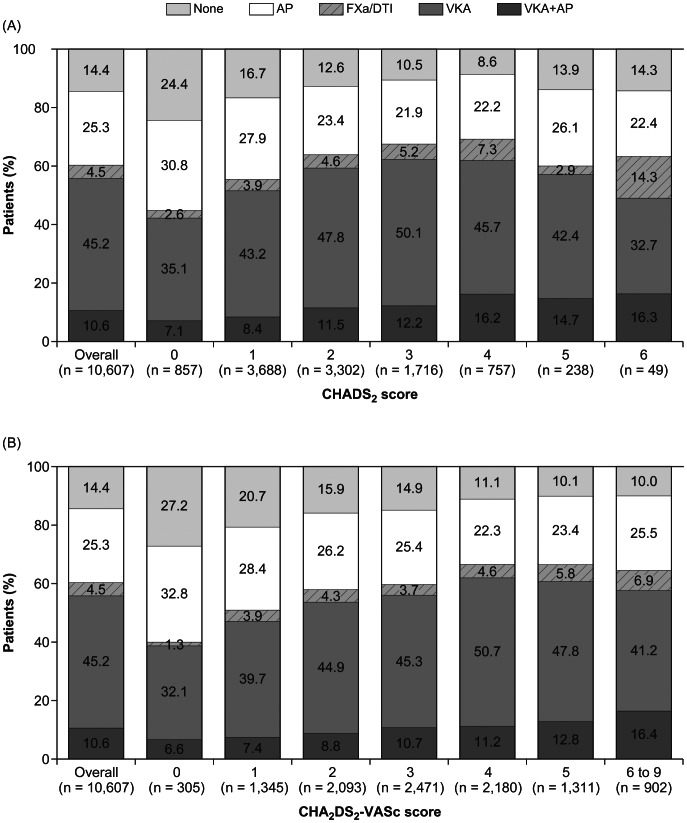
Methods and findings: The Global Anticoagulant Registry in the FIELD (GARFIELD) is an observational study of patients newly diagnosed with non-valvular atrial fibrillation. Enrollment into Cohort 1 (of 5) took place between December 2009 and October 2011 at 540 sites in 19 countries in Europe, Asia-Pacific, Central/South America, and Canada. Investigator sites are representative of the distribution of atrial fibrillation care settings in each country. Cohort 1 comprised 10,614 adults (≥18 years) diagnosed with non-valvular atrial fibrillation within the previous 6 weeks, with ≥1 investigator-defined stroke risk factor (not limited to those in existing risk-stratification schemes), and regardless of therapy. Data collected at baseline included demographics, medical history, care setting, nature of atrial fibrillation, and treatments initiated at diagnosis. The mean (SD) age of the population was 70.2 (11.2) years; 43.2% were women. Mean±SD CHADS2 score was 1.9±1.2, and 57.2% had a score ≥2. Mean CHA2DS2-VASc score was 3.2±1.6, and 8,957 (84.4%) had a score ≥2. Overall, 38.0% of patients with a CHADS2 score ≥2 did not receive anticoagulant therapy, whereas 42.5% of those at low risk (score 0) received anticoagulant therapy.
Conclusions: These contemporary observational worldwide data on non-valvular atrial fibrillation, collected at the end of the vitamin K antagonist-only era, indicate that these drugs are frequently not being used according to stroke risk scores and guidelines, with overuse in patients at low risk and underuse in those at high risk of stroke.
Trial registration: ClinicalTrials.gov TRI08888.
Trial registration: ClinicalTrials.gov NCT01090362.
Conflict of interest statement
Figures
References
-
- Steger C, Pratter A, Martinek-Bregel M, Avanzini M, Valentin A, et al. (2004) Stroke patients with atrial fibrillation have a worse prognosis than patients without: data from the Austrian Stroke registry. Eur Heart J 25: 1734–1740. - PubMed
-
- Kirchhof P, Auricchio A, Bax J, Crijns H, Camm J, et al. (2007) Outcome parameters for trials in atrial fibrillation: executive summary. Eur Heart J 28: 2803–2817. - PubMed
-
- Goto S, Bhatt DL, Rother J, Alberts M, Hill MD, et al... (2008) Prevalence, clinical profile, and cardiovascular outcomes of atrial fibrillation patients with atherothrombosis. Am Heart J 156: 855–863, 863 e852. - PubMed
-
- Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, et al. (2006) ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation-executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients with Atrial Fibrillation). Eur Heart J 27: 1979–2030. - PubMed
-
- Cairns JA, Connolly S, McMurtry S, Stephenson M, Talajic M, et al. (2011) Canadian Cardiovascular Society atrial fibrillation guidelines 2010: prevention of stroke and systemic thromboembolism in atrial fibrillation and flutter. The Canadian journal of cardiology 27: 74–90. - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
