

Mechanical compliance and immunological compatibility of fixative-free decellularized/cryopreserved human pericardium
- PMID: 23705010
- PMCID: PMC3660606
- DOI: 10.1371/journal.pone.0064769
Mechanical compliance and immunological compatibility of fixative-free decellularized/cryopreserved human pericardium
Abstract
Background: The pericardial tissue is commonly used to produce bio-prosthetic cardiac valves and patches in cardiac surgery. The procedures adopted to prepare this tissue consist in treatment with aldehydes, which do not prevent post-graft tissue calcification due to incomplete xeno-antigens removal. The adoption of fixative-free decellularization protocols has been therefore suggested to overcome this limitation. Although promising, the decellularized pericardium has not yet used in clinics, due to the absence of proofs indicating that the decellularization and cryopreservation procedures can effectively preserve the mechanical properties and the immunologic compatibility of the tissue.
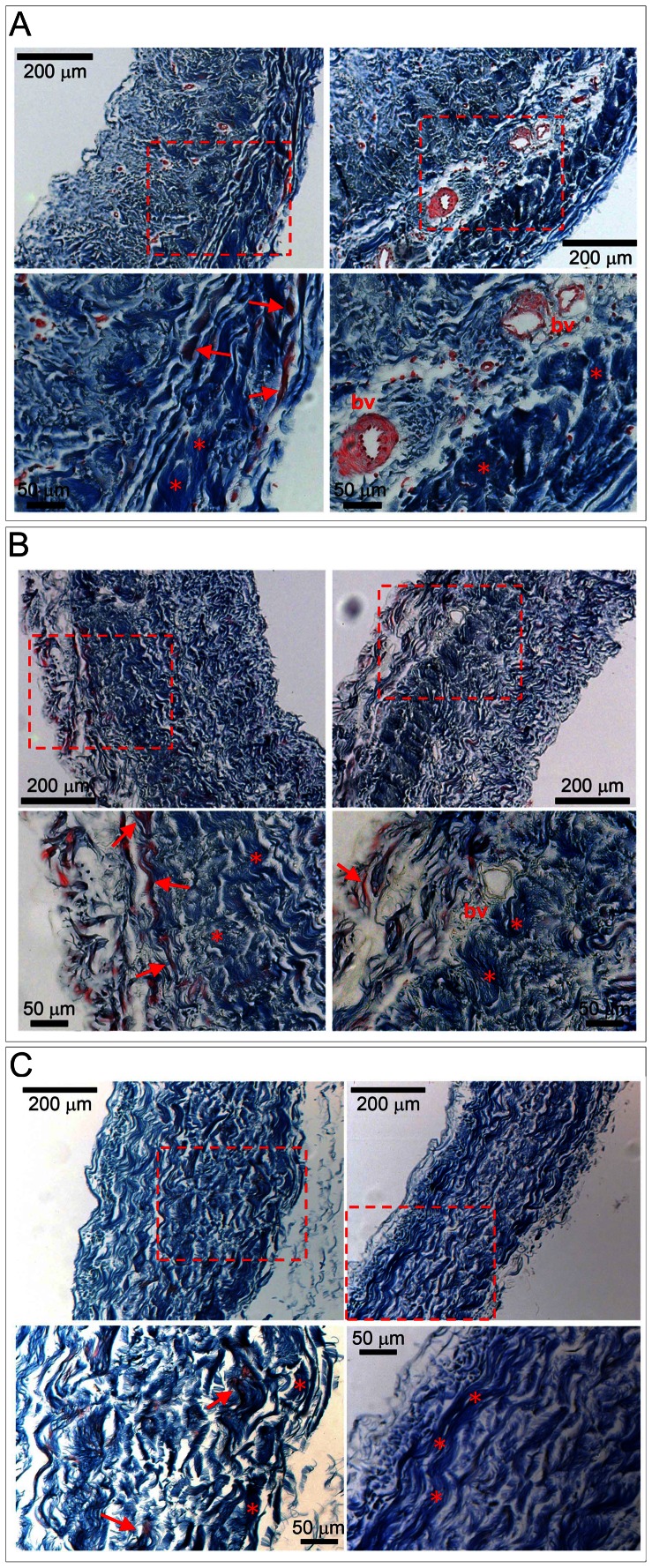
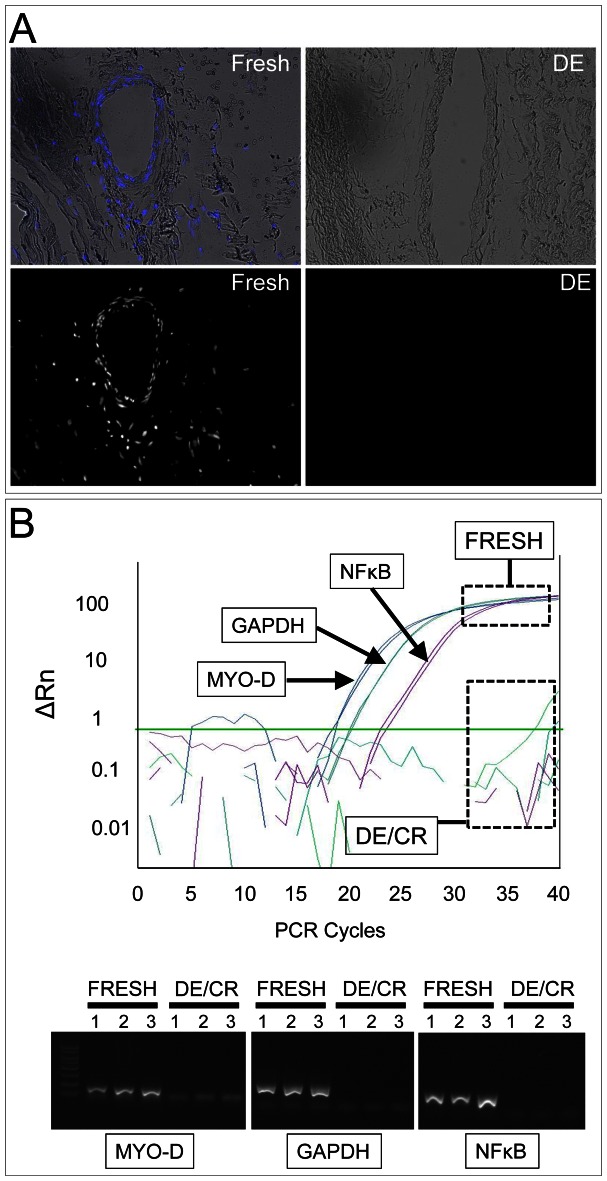
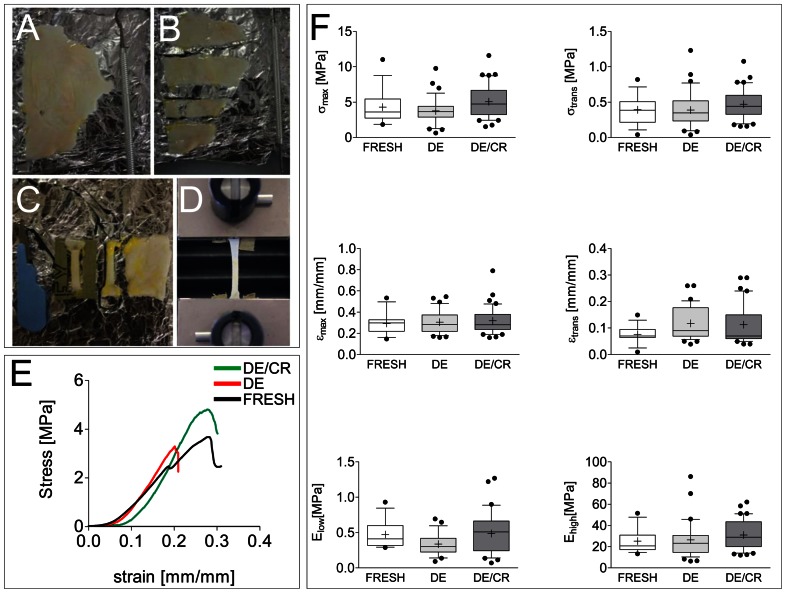
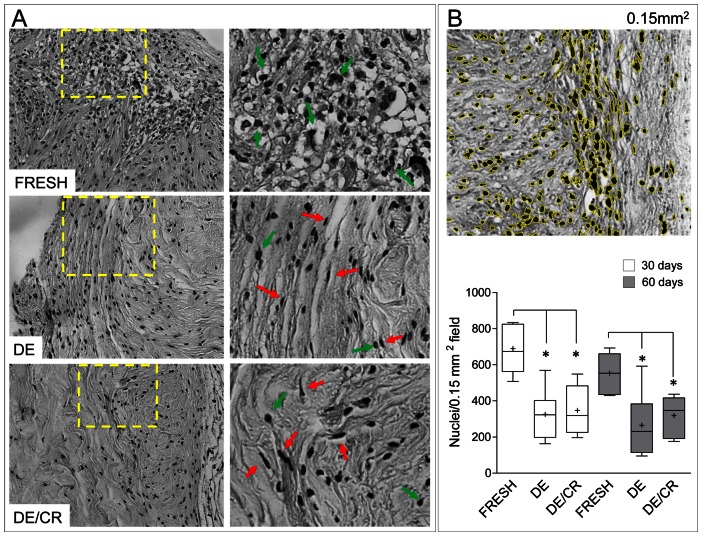
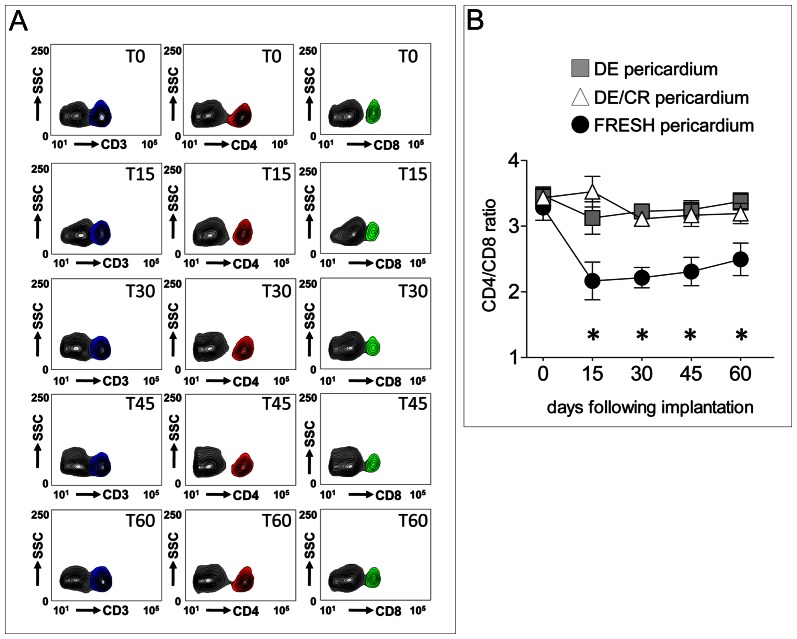
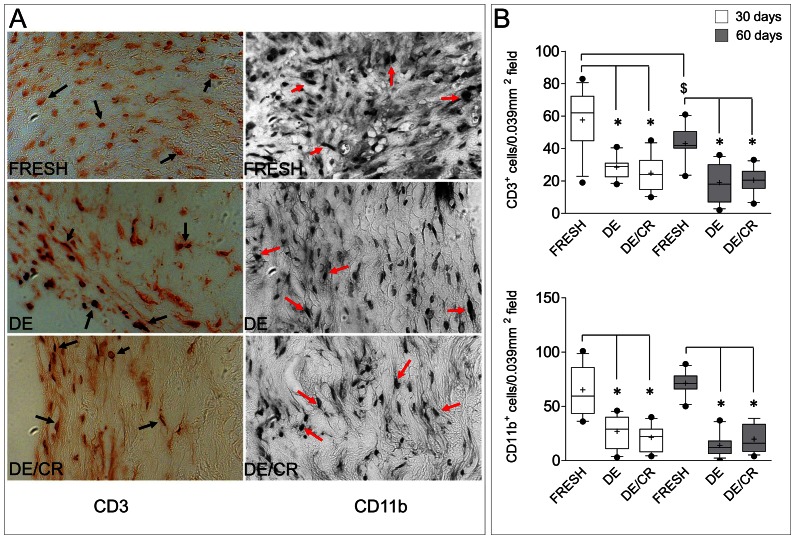
Principal findings: The aim of the present work was to validate a procedure to prepare decellularized/cryopreserved human pericardium which may be implemented into cardiovascular homograft tissue Banks. The method employed to decellularize the tissue completely removed the cells without affecting ECM structure; furthermore, uniaxial tensile loading tests revealed an equivalent resistance of the decellularized tissue to strain, before and after the cryopreservation, in comparison with the fresh tissue. Finally, immunological compatibility, showed a minimized host immune cells invasion and low levels of systemic inflammation, as assessed by tissue transplantation into immune-competent mice.
Conclusions: Our results indicate, for the first time, that fixative-free decellularized pericardium from cadaveric tissue donors can be banked according to Tissue Repository-approved procedures without compromising its mechanical properties and immunological tolerance. This tissue can be therefore treated as a safe homograft for cardiac surgery.
Conflict of interest statement
Figures
References
-
- Carpentier A, Lemaigre G, Robert L, Carpentier S, Dubost C (1969) Biological factors affecting long-term results of valvular heterografts. J Thorac Cardiovasc Surg 58: 467–483. - PubMed
-
- Grabenwoger M, Sider J, Fitzal F, Zelenka C, Windberger U, et al. (1996) Impact of glutaraldehyde on calcification of pericardial bio-prosthetic heart valve material. Ann Thorac Surg 62: 772–777. - PubMed
-
- Vincentelli A, Latremouille C, Zegdi R, Shen M, Lajos PS, et al. (1998) Does glutaraldehyde induce calcification of bio-prosthetic tissues? Ann Thorac Surg 66: S255–258. - PubMed
-
- Bloch O, Golde P, Dohmen PM, Posner S, Konertz W, et al. (2011) Immune response in patients receiving a bio-prosthetic heart valve: lack of response with decellularized valves. Tissue Eng Part A 17: 2399–2405. - PubMed
-
- Galili U (2005) The [alpha]-gal epitope and the anti-Gal antibody in xenotransplantation and in cancer immunotherapy. Immunol Cell Biol 83: 674–686. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
