

Predicting mosquito infection from Plasmodium falciparum gametocyte density and estimating the reservoir of infection
- PMID: 23705071
- PMCID: PMC3660740
- DOI: 10.7554/eLife.00626
Predicting mosquito infection from Plasmodium falciparum gametocyte density and estimating the reservoir of infection
Abstract
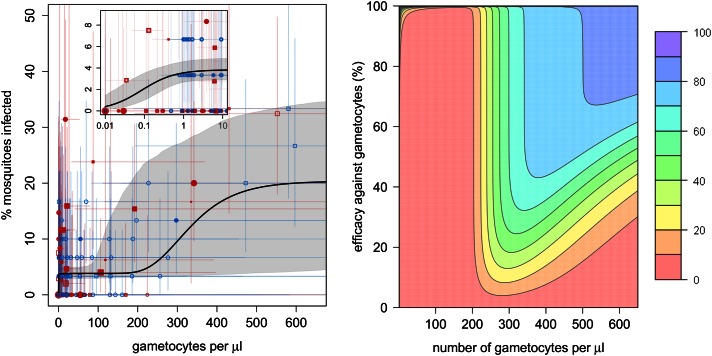
Transmission reduction is a key component of global efforts to control and eliminate malaria; yet, it is unclear how the density of transmission stages (gametocytes) influences infection (proportion of mosquitoes infected). Human to mosquito transmission was assessed using 171 direct mosquito feeding assays conducted in Burkina Faso and Kenya. Plasmodium falciparum infects Anopheles gambiae efficiently at low densities (4% mosquitoes at 1/µl blood), although substantially more (>200/µl) are required to increase infection further. In a site in Burkina Faso, children harbour more gametocytes than adults though the non-linear relationship between gametocyte density and mosquito infection means that (per person) they only contribute slightly more to transmission. This method can be used to determine the reservoir of infection in different endemic settings. Interventions reducing gametocyte density need to be highly effective in order to halt human-mosquito transmission, although their use can be optimised by targeting those contributing the most to transmission. DOI:http://dx.doi.org/10.7554/eLife.00626.001.
Keywords: Gametocyte; Human; Malaria; Mathematical Model; Mosquito; Reservoir of infection.
Conflict of interest statement
The authors declare that no competing interests exist.
Figures

References
-
- Bonnet S, Gouagna LC, Paul RE, Safeukui I, Meunier JY, Boudin C. 2003. Estimation of malaria transmission from humans to mosquitoes in two neighbouring villages in south Cameroon: evaluation and comparison of several indices. Trans R Soc Trop Med Hyg 97:53–9. 10.1016/S0035-9203(03)90022-8 - DOI - PubMed
-
- Boudin C, Lyannaz J, Bosseno MF, Carnevale P, Ambroise-Thomas P. 1991. Epidemiology of Plasmodium falciparum in a rice field and a savanna area in Burkina Faso: seasonal fluctuations of gametocytaemia and malarial infectivity. Ann Trop Med Parasitol 85:377–85 - PubMed
-
- Boudin C, Olivier M, Molez JF, Chiron JP, Ambroise-Thomas P. 1993. High human malarial infectivity to laboratory-bred Anopheles gambiae in a village in Burkina Faso. Am J Trop Med Hyg 48:700–6 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
