

Comparison of symptomatic and asymptomatic atherosclerotic carotid plaques using parallel imaging and 3 T black-blood in vivo CMR
- PMID: 23705576
- PMCID: PMC3693990
- DOI: 10.1186/1532-429X-15-44
Comparison of symptomatic and asymptomatic atherosclerotic carotid plaques using parallel imaging and 3 T black-blood in vivo CMR
Abstract
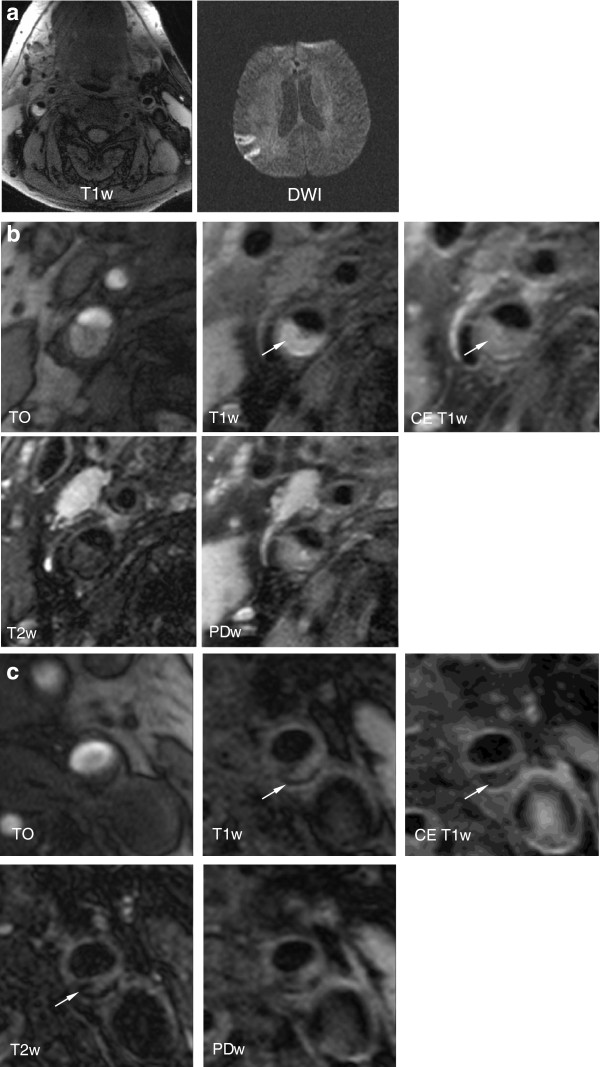
Background: To determine if black-blood 3 T cardiovascular magnetic resonance (bb-CMR) can depict differences between symptomatic and asymptomatic carotid atherosclerotic plaques in acute ischemic stroke patients.
Methods: In this prospective monocentric observational study 34 patients (24 males; 70 ±9.3 years) with symptomatic carotid disease defined as ischemic brain lesions in one internal carotid artery territory on diffusion weighted images underwent a carotid bb-CMR at 3 T with fat-saturated pre- and post-contrast T1w-, PDw-, T2w- and TOF images using surface coils and Parallel Imaging techniques (PAT factor = 2) within 10 days after symptom onset. All patients underwent extensive clinical workup (lab, brain MR, duplex sonography, 24-hour ECG, transesophageal echocardiography) to exclude other causes of ischemic stroke. Prevalence of American Heart Association lesion type VI (AHA-LT6), status of the fibrous cap, presence of hemorrhage/thrombus and area measurements of calcification, necrotic core and hemorrhage were determined in both carotid arteries in consensus by two reviewers who were blinded to clinical information. McNemar and Wilcoxon's signed rank tests were use for statistical comparison. A p-value <0.05 was considered statistically significant.
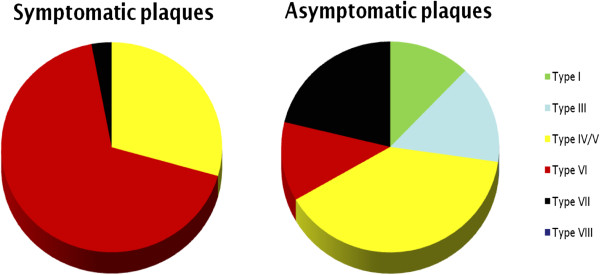
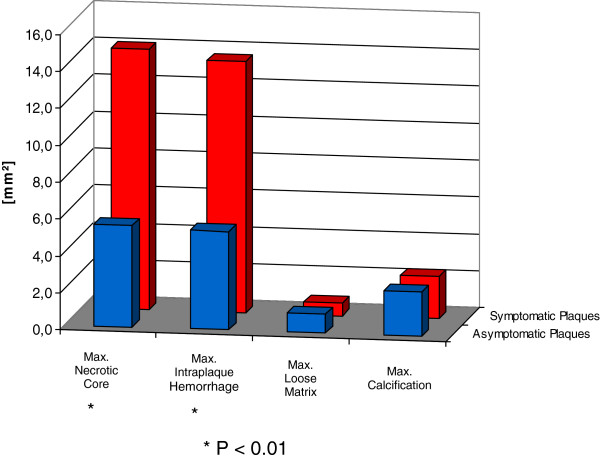
Results: Symptomatic plaques showed a higher prevalence of AHA-LT6 (67.7% vs. 11.8%; p < 0.001; odds ratio = 12.5), ruptured fibrous caps (44.1% vs. 2.9%; p < 0.001; odds ratio = 15.0), juxtaluminal thrombus (26.5 vs. 0%; p < 0.01; odds ratio = 7.3) and intraplaque hemorrhage (58.6% vs. 11.8%; p = 0.01; odds ratio = 3.8). Necrotic core and hemorrhage areas were greater in symptomatic plaques (14.1 mm2 vs. 5.5 mm2 and 13.6 mm2 vs. 5.3 mm2; p < 0.01, respectively).
Conclusion: 3 T bb-CMR is able to differentiate between symptomatic and asymptomatic carotid plaques, demonstrating the potential of bb-CMR to differentiate between stable and vulnerable lesions and ultimately to identify patients with low versus high risk for cardiovascular complications. Best predictors of the symptomatic side were a ruptured fibrous cap, AHA-LT 6, juxtaluminal hemorrhage/thrombus, and intraplaque hemorrhage.
Figures
References
-
- Goldstein LB, Bushnell CD, Adams RJ, Appel LJ, Braun LT, Chaturvedi S, Creager MA, Culebras A, Eckel RH, Hart RG. Guidelines for the primary prevention of stroke: a guideline for healthcare professionals from the american heart association/american stroke association. Stroke. 2011;42:517–584. doi: 10.1161/STR.0b013e3181fcb238. - DOI - PubMed
-
- Hellings WE, Peeters W, Moll FL, Piers SR, van Setten J, Van der Spek PJ, de Vries JP, Seldenrijk KA, De Bruin PC, Vink A. Composition of carotid atherosclerotic plaque is associated with cardiovascular outcome: a prognostic study. Circulation. 2010;121:1941–1950. doi: 10.1161/CIRCULATIONAHA.109.887497. - DOI - PubMed
-
- Makino K, Yoshitama T, Kanda S, Takasawa Y, Yamada T, Itaya H, Lee T, Saeki F, Nakamura M, Sugi K. Relation of coronary plaque composition determined by 64-slice multidetector computed tomography in patients with suspected coronary heart disease. Am J Cardiol. 2011;107:1624–1629. doi: 10.1016/j.amjcard.2011.01.047. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
