

Clinical results of XMR-assisted percutaneous transforaminal endoscopic lumbar discectomy
- PMID: 23705685
- PMCID: PMC3668223
- DOI: 10.1186/1749-799X-8-14
Clinical results of XMR-assisted percutaneous transforaminal endoscopic lumbar discectomy
Abstract
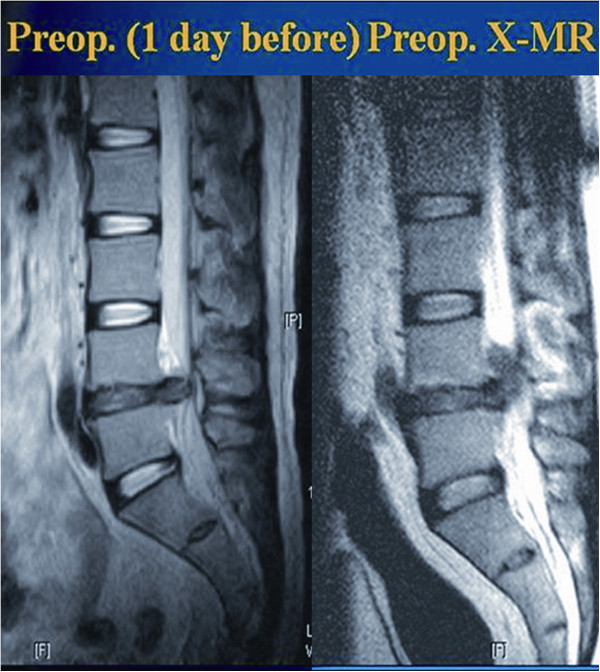
Background: Although percutaneous endoscopic lumbar discectomy (PELD) has shown favorable outcomes in the majority of lumbar discectomy cases, there were also some failures. The most common cause of failure is the incomplete removal of disc fragments. The skin entry point for the guide-needle trajectory and the optimal placement of the working sleeve are largely blind, which might lead to the inadequate removal of disc fragments. The objective of this study was to present our early experiences with image-guided PELD using a specially designed fluoroscope with magnetic resonance imaging-equipped operative suite (XMR) for the treatment of lumbar disc herniation.
Methods: This prospective study included 89 patients who had undergone PELD via the transforaminal approach using an XMR protocol. Pre- and postoperative examinations (at 12 weeks) included a detailed clinical history, visual analogue scale (VAS), Oswestry disability index (ODI), and radiological workups. The results were categorized as excellent, good, fair, and poor according to MacNab's criteria. At the final follow-up, the minimum follow-up time for the subjects was 2 years. The need for revision surgeries and postoperative complications were noted on follow-up.
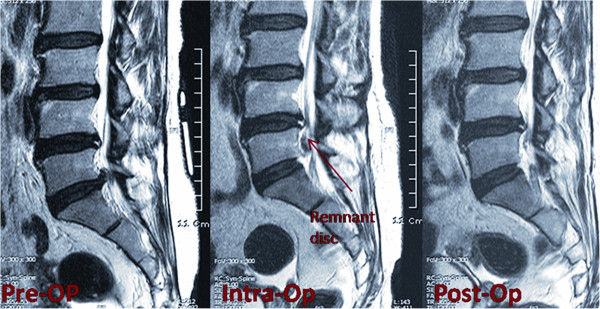
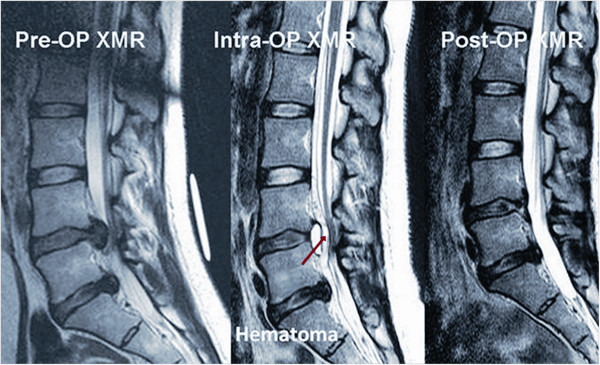
Results: Postoperative mean ODI decreased from 67.4% to 5.61%. Mean VAS score for back and leg pain improved significantly from 4 to 2.3 and from 7.99 to 1.04, respectively. Four (4.49%) patients underwent a second-stage PELD after intraoperative XMR had shown remnant fragments after the first stage. As per MacNab's criteria, 76 patients (85.4%) showed excellent, 8 (8.89%) good, 3 (3.37%) fair, and 2 (2.25) poor results. Four (4.49%) patients had remnant disc fragments on XMR, which were removed during the same procedure. All of these patients had either highly migrated or sequestrated disc fragments preoperatively. Four (4.49%) other patients needed a second, open surgery due to symptomatic postoperative hematoma (n = 2) and recurrent disc herniation (n = 2).
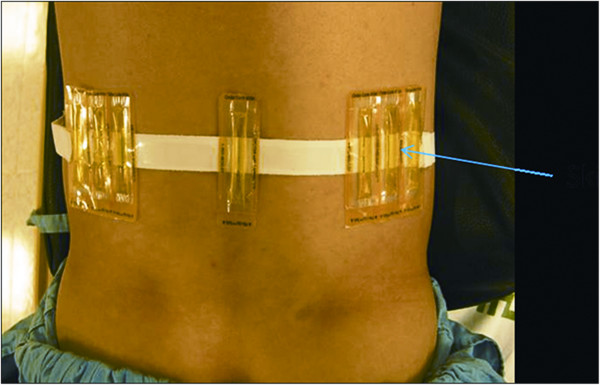
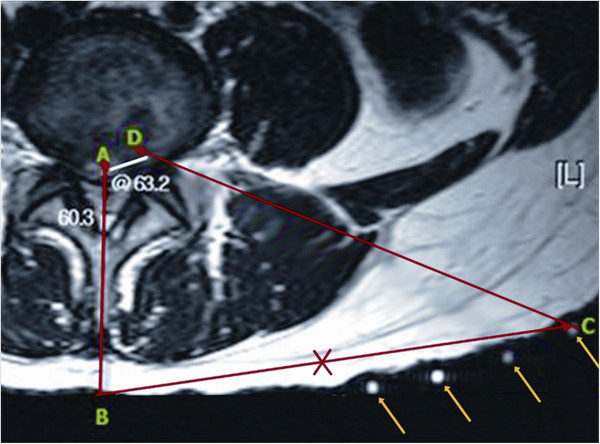
Conclusions: This prospective analysis indicates that XMR-assisted PELD provides a precise skin entry point. It also confirms that decompression occurs intraoperatively, which negates the need for a separate surgery and thus increases the success rate of PELD, particularly in highly migrated or sequestrated discs. However, further extensive experience is required to confirm the advantages and feasibility of PELD in terms of cost effectiveness.
Figures

References
-
- Brotchi J, Pirotte B, De Witte O. Prevention of epidural fibrosis in a prospective series of 100 primary lumbo-sacral discectomy patients: follow-up and assessment at re-operation. Neurol Res. 1999;21:S47–S50. - PubMed
-
- Maroon J, Abla A, Bost J. Association between peridural scar and persistant low back pain after lumbar discectomy. Neurol Res. 1999;21:S43–S46. - PubMed
-
- Dunlop R, Adams M, Hutton W. Disc space narrowing and lumbar facet joints. J Bone Joint Surg Br. 1984;66:706–710. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
